

Is the Lung Built for Exercise? Advances and Unresolved Questions
- PMID: 37443459
- PMCID: PMC11186580
- DOI: 10.1249/MSS.0000000000003255
Is the Lung Built for Exercise? Advances and Unresolved Questions
Abstract
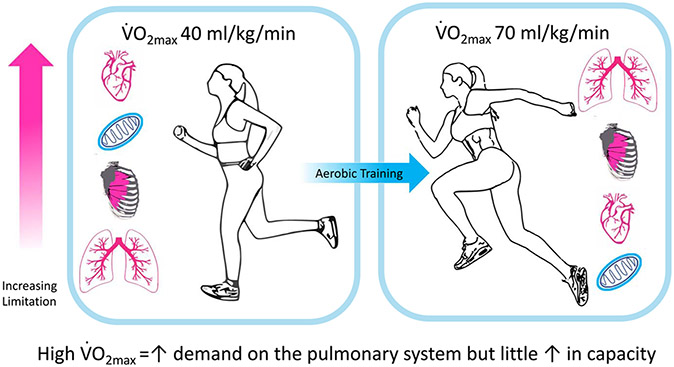
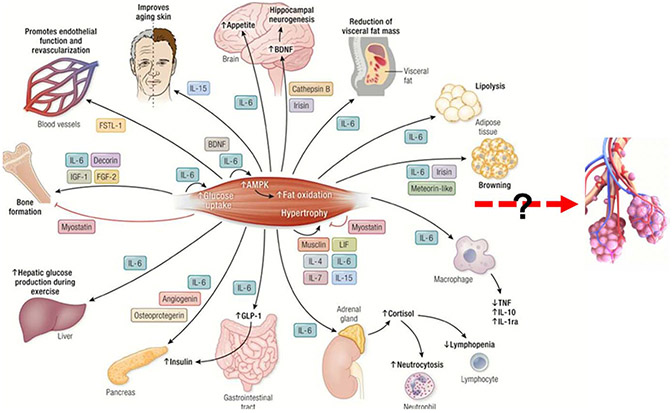
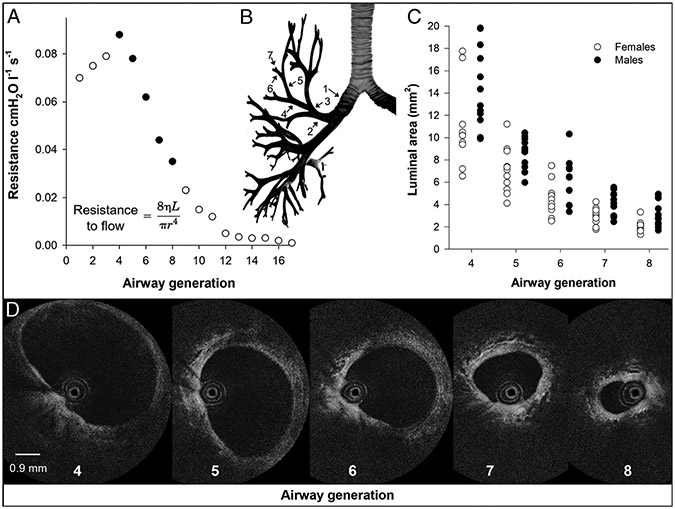
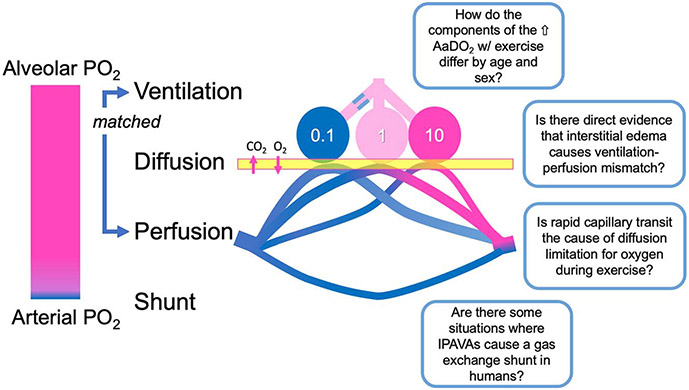
Nearly 40 yr ago, Professor Dempsey delivered the 1985 ACSM Joseph B. Wolffe Memorial Lecture titled: "Is the lung built for exercise?" Since then, much experimental work has been directed at enhancing our understanding of the functional capacity of the respiratory system by applying complex methodologies to the study of exercise. This review summarizes a symposium entitled: "Revisiting 'Is the lung built for exercise?'" presented at the 2022 American College of Sports Medicine annual meeting, highlighting the progress made in the last three-plus decades and acknowledging new research questions that have arisen. We have chosen to subdivide our topic into four areas of active study: (i) the adaptability of lung structure to exercise training, (ii) the utilization of airway imaging to better understand how airway anatomy relates to exercising lung mechanics, (iii) measurement techniques of pulmonary gas exchange and their importance, and (iv) the interactions of the respiratory and cardiovascular system during exercise. Each of the four sections highlights gaps in our knowledge of the exercising lung. Addressing these areas that would benefit from further study will help us comprehend the intricacies of the lung that allow it to meet and adapt to the acute and chronic demands of exercise in health, aging, and disease.
Copyright © 2023 by the American College of Sports Medicine.
Figures
Similar articles
-
J.B. Wolffe memorial lecture. Is the lung built for exercise?Med Sci Sports Exerc. 1986 Apr;18(2):143-55. Med Sci Sports Exerc. 1986. PMID: 3517547 Review.
-
The pulmonary system during exercise in hypoxia and the cold.Exp Physiol. 2010 Mar;95(3):422-30. doi: 10.1113/expphysiol.2009.047571. Epub 2009 Oct 23. Exp Physiol. 2010. PMID: 19854797 Review.
-
Demand vs. capacity in the healthy pulmonary system.Schweiz Z Sportmed. 1992 Jun;40(2):55-64. Schweiz Z Sportmed. 1992. PMID: 1626272 Review.
-
Extracorporeal lung support technologies - bridge to recovery and bridge to lung transplantation in adult patients: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(5):1-47. Epub 2010 Apr 1. Ont Health Technol Assess Ser. 2010. PMID: 23074408 Free PMC article.
-
J.B. Wolffe Memorial Lecture. Health consequences of physical activity: understanding and challenges regarding dose-response.Med Sci Sports Exerc. 1994 Jun;26(6):649-60. doi: 10.1249/00005768-199406000-00001. Med Sci Sports Exerc. 1994. PMID: 8052103
Cited by
-
Lack of sex-specific differences in the associations between the dimensions of great vessels and exercise performance in amateur cyclists.PLoS One. 2024 Nov 4;19(11):e0313165. doi: 10.1371/journal.pone.0313165. eCollection 2024. PLoS One. 2024. PMID: 39495753 Free PMC article.
-
Test-retest reliability of cardiopulmonary exercise test-derived metrics in individuals with COPD versus healthy controls.Clin Physiol Funct Imaging. 2025 Jan;45(1):e12927. doi: 10.1111/cpf.12927. Clin Physiol Funct Imaging. 2025. PMID: 39878361 Free PMC article.
-
Assessing the repeatability of expiratory flow limitation during incremental exercise in healthy adults.Physiol Rep. 2024 Oct;12(19):e70068. doi: 10.14814/phy2.70068. Physiol Rep. 2024. PMID: 39358859 Free PMC article.
-
Cardiac output limits maximal oxygen consumption, but what limits maximal cardiac output?Exp Physiol. 2025 May;110(5):666-674. doi: 10.1113/EP091594. Epub 2025 Apr 7. Exp Physiol. 2025. PMID: 40193294 Free PMC article. Review.
-
The Effect of Aerobic Training on Healthy Small Airways-A Forced Oscillation Technique Approach to Optimize Long Term Care in COPD.J Clin Med. 2025 Jul 4;14(13):4755. doi: 10.3390/jcm14134755. J Clin Med. 2025. PMID: 40649129 Free PMC article.
References
-
- Dempsey JA. J.B. Wolffe memorial lecture. Is the lung built for exercise? Med Sci Sports Exerc. 1986;18(2):143–55. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
