

Intradiscal Gelified Ethanol Nucleolysis versus Endoscopic Surgery for Lumbar Disc Herniation Radiculopathy
- PMID: 37443558
- PMCID: PMC10341163
- DOI: 10.3390/diagnostics13132164
Intradiscal Gelified Ethanol Nucleolysis versus Endoscopic Surgery for Lumbar Disc Herniation Radiculopathy
Abstract
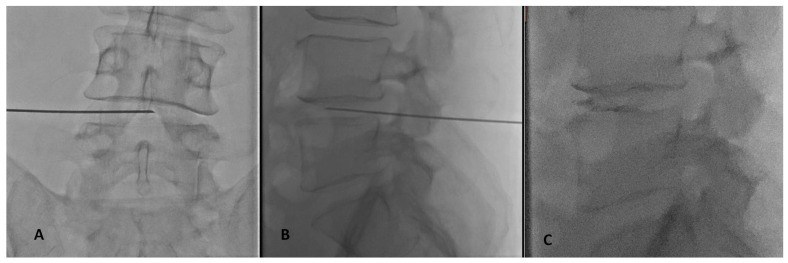
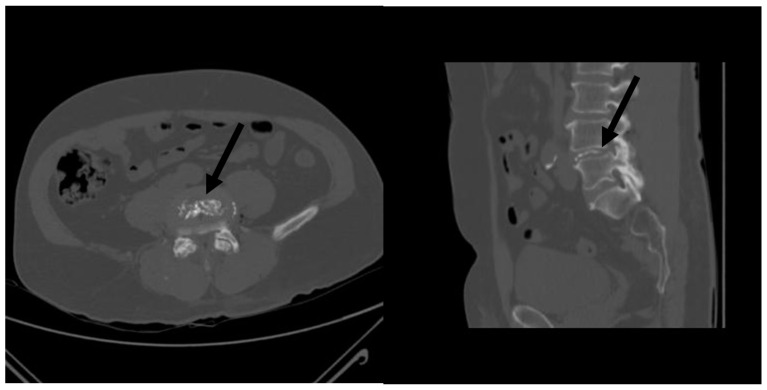
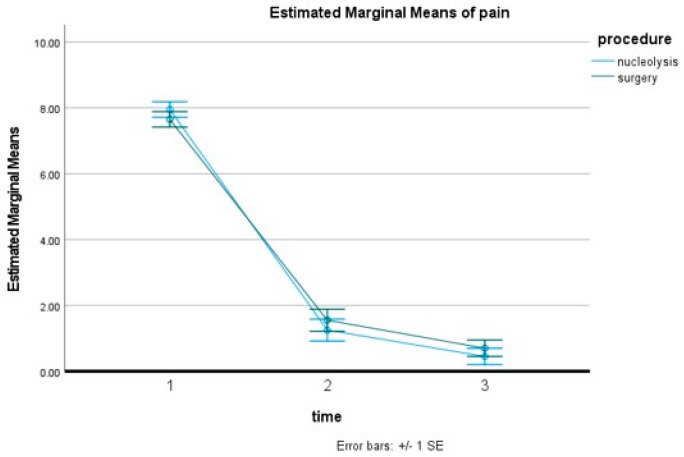
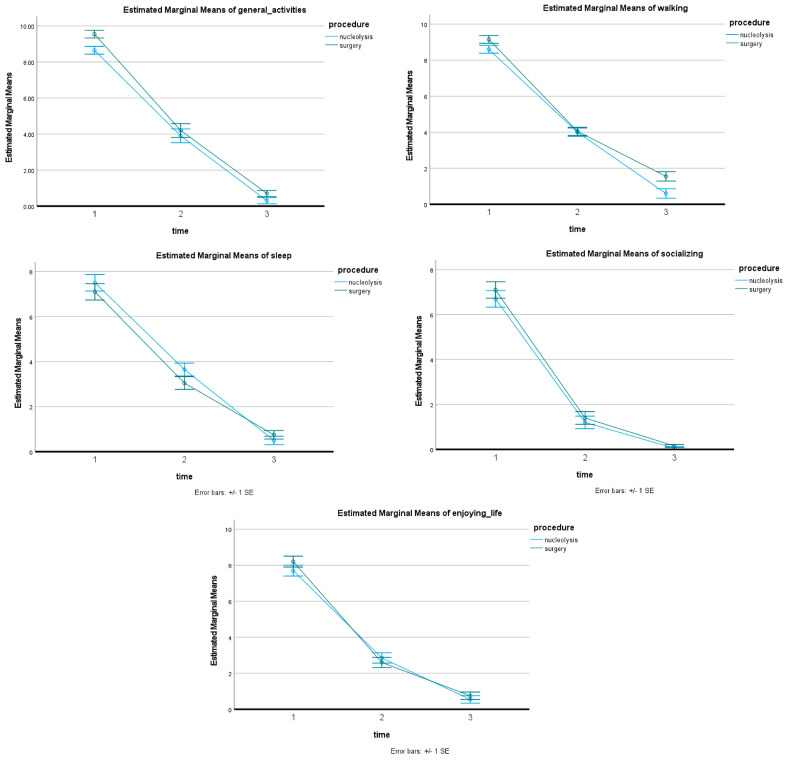
The purpose of this study was to retrospectively compare efficacy and safety between intradiscal injection of a gelified ethanol product and tubular discectomy in the treatment of intervertebral disk herniation. A bi-central institutional database research identified forty (40) patients suffering from symptomatic contained disc herniation. Nucleolysis Group included 20 patients [mean 50.05 ± 9.27 years-of-age (male/female 14/6-70/30%)] and Surgery Group included 20 patients [mean 48.45 ± 14.53 years-of-age, (male/female 12/8-60/40%)]. Primary outcome was overall 12-month improvement over baseline in leg pain (NVS units). Procedural technical outcomes were recorded, and adverse events were evaluated at all follow-up intervals. CIRSE classification system was used for complications' reporting. Mean pre-operative pain score in Nucleolysis Group was 7.95 ± 0.94 reduced to 1.25 ± 1.11 at month 1 and 0.45 ± 0.75 NVS units at year 1. Mean pre-operative pain score in Surgery Group was 7.65 ± 1.13 reduced to 1.55 ± 1.79 at month 1 and 0.70 ± 1.38 NVS units at year 1. Pain decrease was statistically significant after both procedures (p < 0.001). There was no statistically significant difference between pain reduction in both groups (p = 0.347). The decrease differences of the pain effect upon general activities, sleeping, socializing, walking, and enjoying life in the follow-up period between the two groups were not statistically significant. No complications were noted in both groups. Results from the current study report that intradiscal injection of a gelified ethanol and tubular discectomy were equally effective on terms of efficacy and safety for the treatment of symptomatic lumbar intervertebral disc herniation regarding the 12-month mean leg pain improvement. Both achieved similar rapid significant clinical improvement persisting throughout follow-up period.
Keywords: alcohol; herniation; injection; intervertebral disc; pain; tubular discectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
