

Orthodontic and Facial Characteristics of Craniofacial Syndromic Children with Obstructive Sleep Apnea
- PMID: 37443607
- PMCID: PMC10340152
- DOI: 10.3390/diagnostics13132213
Orthodontic and Facial Characteristics of Craniofacial Syndromic Children with Obstructive Sleep Apnea
Abstract
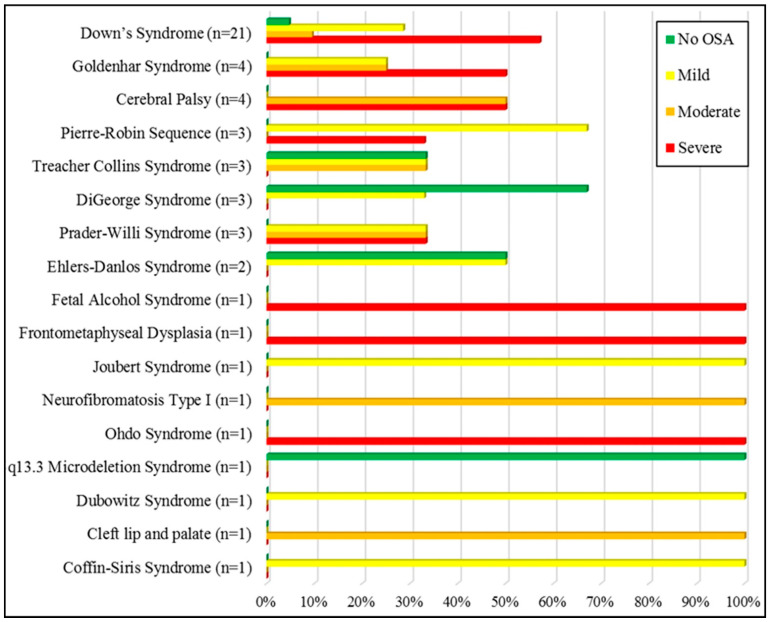
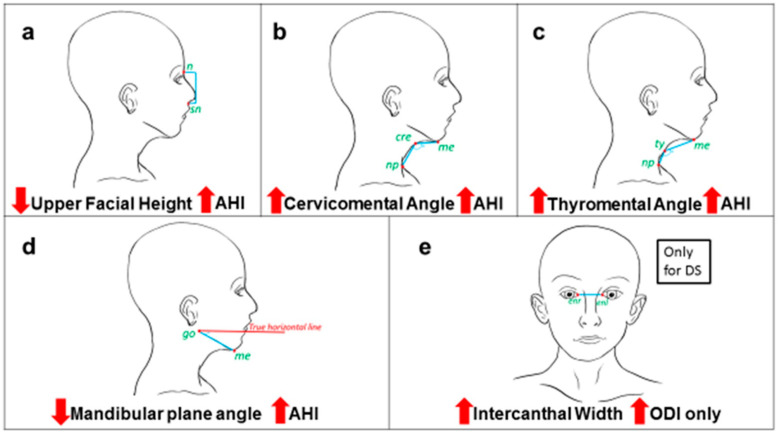
Introduction: Obstructive sleep apnea (OSA) is a disorder in which ventilation becomes disrupted due to a complete or partial upper airway obstruction Altered craniofacial morphology is one of the most important anatomical factors associated with obstructive sleep apnea (OSA). Studies have assessed craniofacial features in the non-syndromic pediatric population. The aim of this study was to analyze the orthodontic and facial characteristic of craniofacial syndromic children referred for polysomnography (PSG) and to assess the correlation with the apnea-hypopnea index (AHI). Methods: In the current cross-sectional study, consecutive syndromic patients referred for PSG were invited to participate. A systematic clinical examination including extra- and intra-oral orthodontic examination was performed by calibrated orthodontists. Standardized frontal and profile photographs with reference points were taken and analyzed using ImageJ® software to study the craniofacial morphology. PSG data were analyzed for correlation with craniofacial features. STROBE guidelines were strictly adopted during the research presentation. Results: The sample included 52 syndromic patients (50% females, mean age 9.38 ± 3.36 years) diagnosed with 17 different syndromes, of which 24 patients had craniofacial photography analysis carried out. Most of the sample (40%) had severe OSA, while only 5.8% had no OSA. Down's syndrome (DS) was the most common syndrome (40%) followed by Goldenhar syndrome (5%), Pierre Robin Sequence (5%), and other syndromes. The severity of AHI was significantly correlated with decreased midfacial height. increased thyromental angle and cervicomental angle, decreased mandibular angle, and decreased upper facial height. All patients with DS were diagnosed with OSA (57% severe OSA), and their ODI was significantly correlated with increased intercanthal distance. Obesity was not correlated to the severity of AHI for syndromic patients. Conclusions: Decreased midfacial height and obtuse thyromental angle were correlated with increased AHI for syndromic patients. Increased intercanthal distance of DS patients could be a major predictor of OSA severity. Obesity does not seem to play a major role in the severity of OSA for syndromic patients. Further studies with larger samples are necessary to confirm these findings.
Keywords: apnea–hypopnea index; diagnostic imaging; pediatric; polysomnography; syndromes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Li H.-Y., Lee L.-A. Sleep-disordered breathing in children. Chang. Gung Med. J. 2009;32:247–257. - PubMed
-
- Sheldon S.H., Ferber R., Kryger M.H. Principles and Practice of Pediatric Sleep Medicine. Elsevier Health Sciences; Amsterdam, The Netherlands: 2005.
-
- Kheirandish-Gozal L., Gozal D. Sleep Disordered Breathing in Children: A Comprehensive Clinical Guide to Evaluation and Treatment. Springer Science & Business Media; Cham, Switzerland: 2012.
LinkOut - more resources
Full Text Sources
