

Native T2 Predicts Myocardial Inflammation Irrespective of a Patient's Volume Status
- PMID: 37443634
- PMCID: PMC10340351
- DOI: 10.3390/diagnostics13132240
Native T2 Predicts Myocardial Inflammation Irrespective of a Patient's Volume Status
Abstract
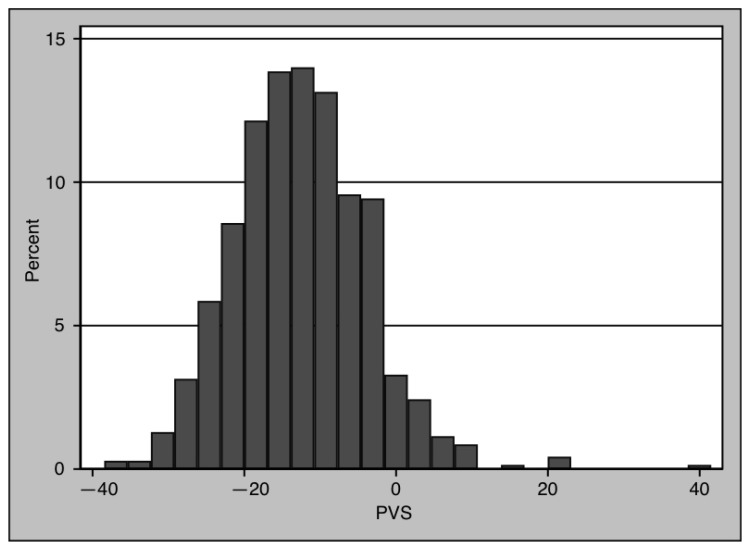
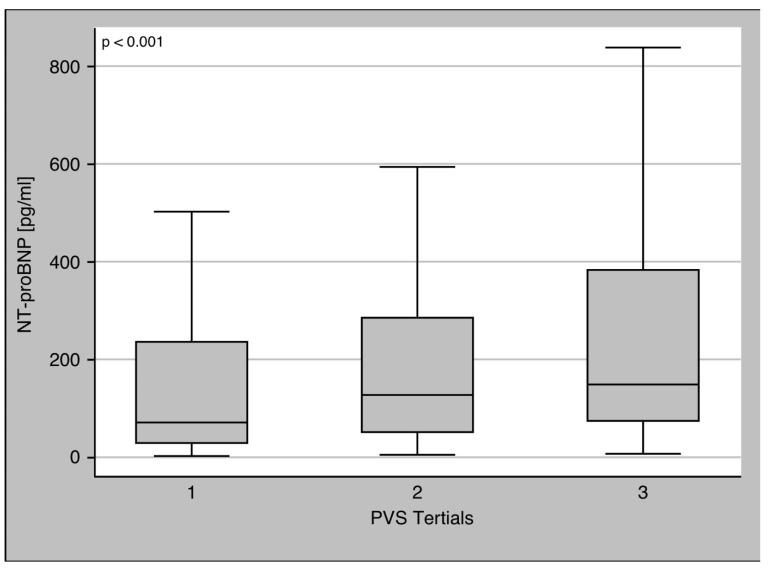
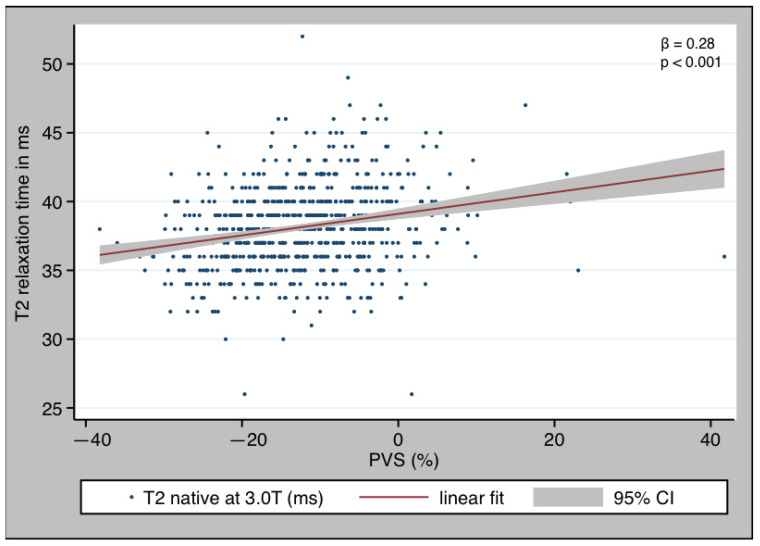
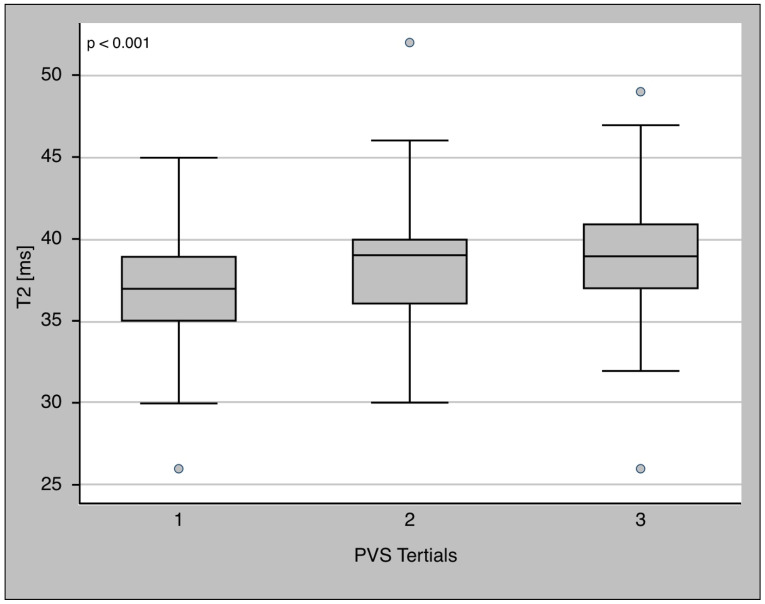
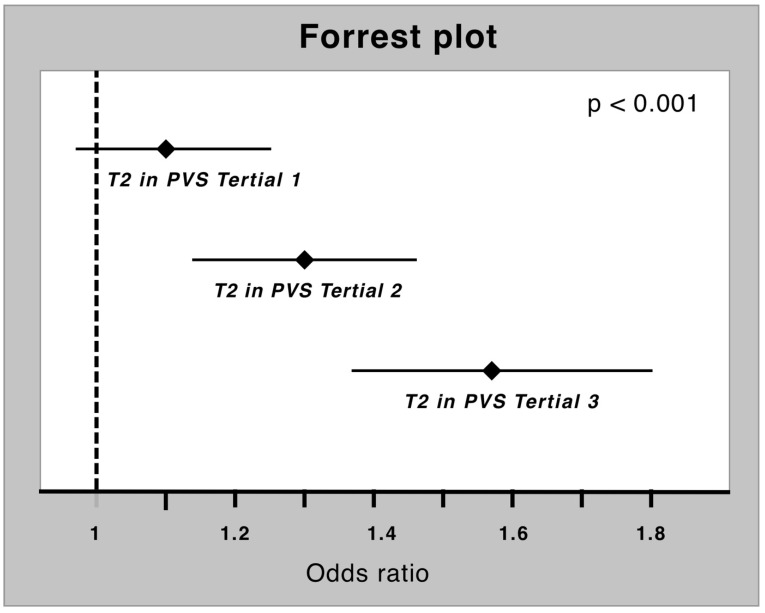
Myocardial inflammation and edema are major pathological features in myocarditis. Myocardial tissue water content and myocardial edema can be quantified via T2 mapping. Thus, cardiac magnetic resonance (CMR) is the noninvasive gold standard for diagnosing myocarditis. Several studies showed an impact of short-term volume changes on T2 relaxation time. Plasma volume status (PVS) is a good surrogate parameter to quantify a patient's volume status, and it is simple to use. The aim of this study was to determine the effect of PVS on the diagnostic value of T2 relaxation time in myocardial inflammation. Between April 2017 and December 2022, patients who were indicated for cardiac CMR were included in our prospective clinical registry. Patients with myocardial inflammation and those with unremarkable findings were analyzed in the present study. A blood sample was drawn, and PVS was calculated. Patients were separated into PVS tertiles to explore a possible nonlinear dose-response relationship. Logistic regression analysis was used to determine whether T2 is an independent predictor of myocardial inflammation. A total of 700 patients (47.43% female) were eligible for analysis. Of these, 551 patients were healthy (78.7%), while 149 (21.3%) showed signs of myocardial inflammation. The T2 relaxation time was elevated in patients with myocardial inflammation (40 ms [IQR 37-42 ms] vs. 38.0 ms [IQR 36-39 ms], p < 0.001). PVS showed no difference between the groups (-12.94 [IQR -18.4--7.28] vs.-12.19 [IQR -18.93--5.87], p = 0.384). T2 showed a clear dose-response relationship with PVS, with increasing T2 values along the PVS tertiles. In spite of this, T2 was found to be an independent marker of myocardial inflammation in logistic regression (OR T2 1.3 [95% CI 1.21-1.39], p < 0.001), even after adjusting for PVS (OR T2 [adj. PVS] 1.31 [95% CI 1.22-1.40], p < 0.001). Despite a dose-response relationship between T2 and the volume status, T2 was found to be an independent indicator of myocardial inflammation.
Keywords: CMR; PVS; T2; myocardial inflammation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ammirati E., Cipriani M., Moro C., Raineri C., Pini D., Sormani P., Mantovani R., Varrenti M., Pedrotti P., Conca C., et al. Clinical Presentation and Outcome in a Contemporary Cohort of Patients With Acute Myocarditis: Multicenter Lombardy Registry. Circulation. 2018;138:1088–1099. doi: 10.1161/CIRCULATIONAHA.118.035319. - DOI - PubMed
-
- Tschöpe C., Ammirati E., Bozkurt B., Caforio A.L.P., Cooper L.T., Felix S.B., Hare J.M., Heidecker B., Heymans S., Hübner N., et al. Myocarditis and Inflammatory Cardiomyopathy: Current Evidence and Future Directions. Nat. Rev. Cardiol. 2021;18:169–193. doi: 10.1038/s41569-020-00435-x. - DOI - PMC - PubMed
-
- Global Burden of Disease Study 2013 Collaborators Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990-2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. doi: 10.1016/S0140-6736(15)60692-4. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
