

Sleep-Disordered Breathing and Prognosis after Ischemic Stroke: It Is Not Apnea-Hypopnea Index That Matters
- PMID: 37443640
- PMCID: PMC10340264
- DOI: 10.3390/diagnostics13132246
Sleep-Disordered Breathing and Prognosis after Ischemic Stroke: It Is Not Apnea-Hypopnea Index That Matters
Abstract
Background: Sleep-disordered breathing (SDB) is highly prevalent after stroke and is considered to be a risk factor for poor post-stroke outcomes. The aim of this observational study was to evaluate the effect of nocturnal respiratory-related indices based on nocturnal respiratory polygraphy on clinical outcomes (including mortality and non-fatal events) in patients with ischemic stroke.
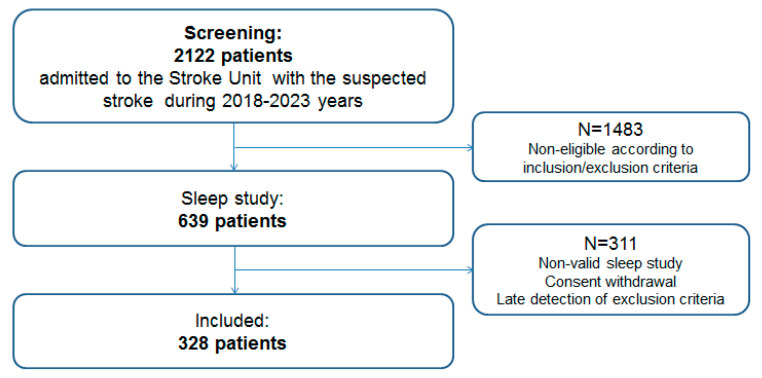
Methods: A total of 328 consecutive patients (181 (55%) males, mean age 65.8 ± 11.2 years old) with confirmed ischemic stroke admitted to a stroke unit within 24 h after stroke onset were included in the analysis. All patients underwent standard diagnostic and treatment procedures, and sleep polygraphy was performed within the clinical routine in the first 72 h after admission. The long-term outcomes were assessed by cumulative endpoint (death of any cause, new non-fatal myocardial infarction, new non-fatal stroke/transient ischemic attack, emergency revascularization, emergency hospitalization due to the worsening of cardiovascular disease). A Cox-regression analysis was applied to evaluate the effects of nocturnal respiratory indices on survival.
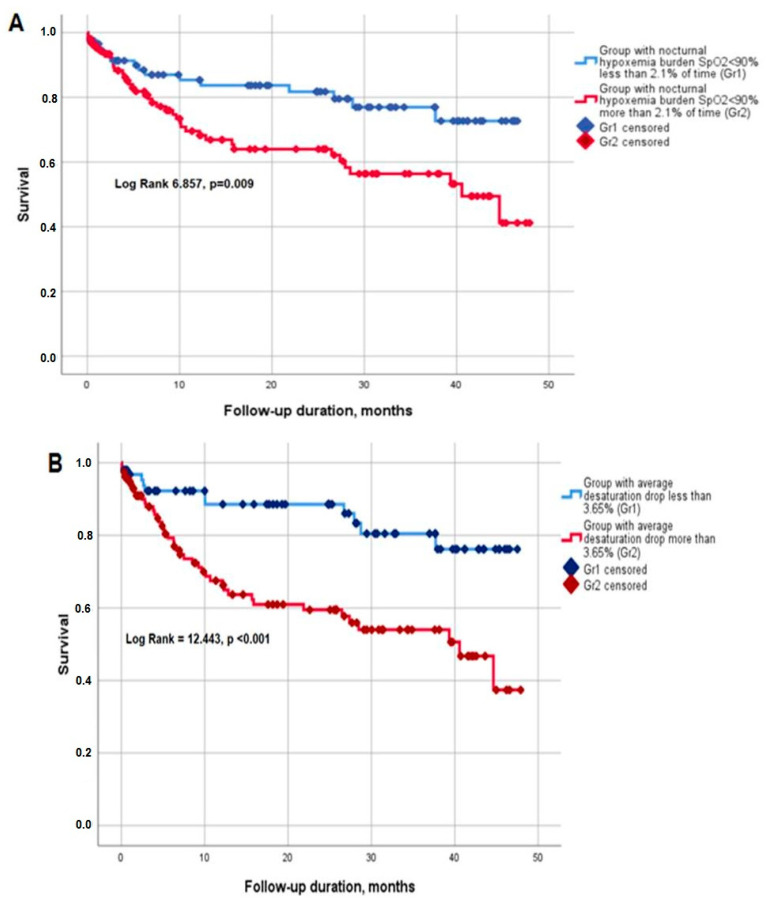
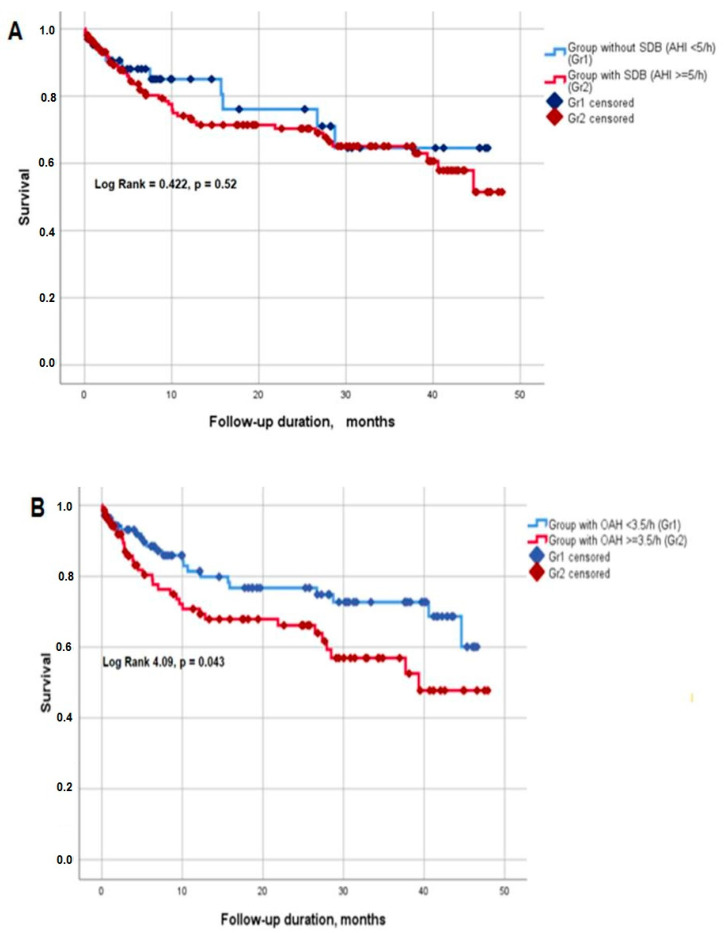
Results: The mean follow-up period comprised 12 months (maximal-48 months). Patients with unfavourable outcomes demonstrated a higher obstructive apnea-hypopnea index, a higher hypoxemia burden assessed as a percent of the time with SpO2 < 90%, a higher average desaturation drop, and a higher respiratory rate at night. Survival time was significantly lower (30.6 (26.5; 34.7) versus 37.9 (34.2; 41.6) months (Log Rank 6.857, p = 0.009)) in patients with higher hypoxemia burden (SpO2 < 90% during ≥2.1% versus <2.1% of total analyzed time). However, survival time did not differ depending on the SDB presence assessed by AHI thresholds (either ≥5 or ≥15/h). The multivariable Cox proportional hazards regression (backward stepwise analysis) model demonstrated that the parameters of hypoxemia burden were significantly associated with survival time, independent of age, stroke severity, stroke-related medical interventions, comorbidities, and laboratory tests.
Conclusion: Our study demonstrates that the indices of hypoxemia burden have additional independent predictive value for long-term outcomes (mortality and non-fatal cardiovascular events) after ischemic stroke.
Keywords: hypoxemia burden; ischemic stroke; sleep-disordered breathing; stroke; stroke outcome.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Feigin V.L., Stark B.A., Johnson C.O., Roth G.A., Bisignano C., Abady G.G., Abbasifard M., Abbasi-Kangevari M., Abd-Allah F., Abedi V., et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20:795–820. doi: 10.1016/S1474-4422(21)00252-0. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
