

Omitting Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy for Clinically Node Negative HER2 Positive and Triple Negative Breast Cancer: A Pooled Analysis
- PMID: 37444434
- PMCID: PMC10340379
- DOI: 10.3390/cancers15133325
Omitting Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy for Clinically Node Negative HER2 Positive and Triple Negative Breast Cancer: A Pooled Analysis
Abstract
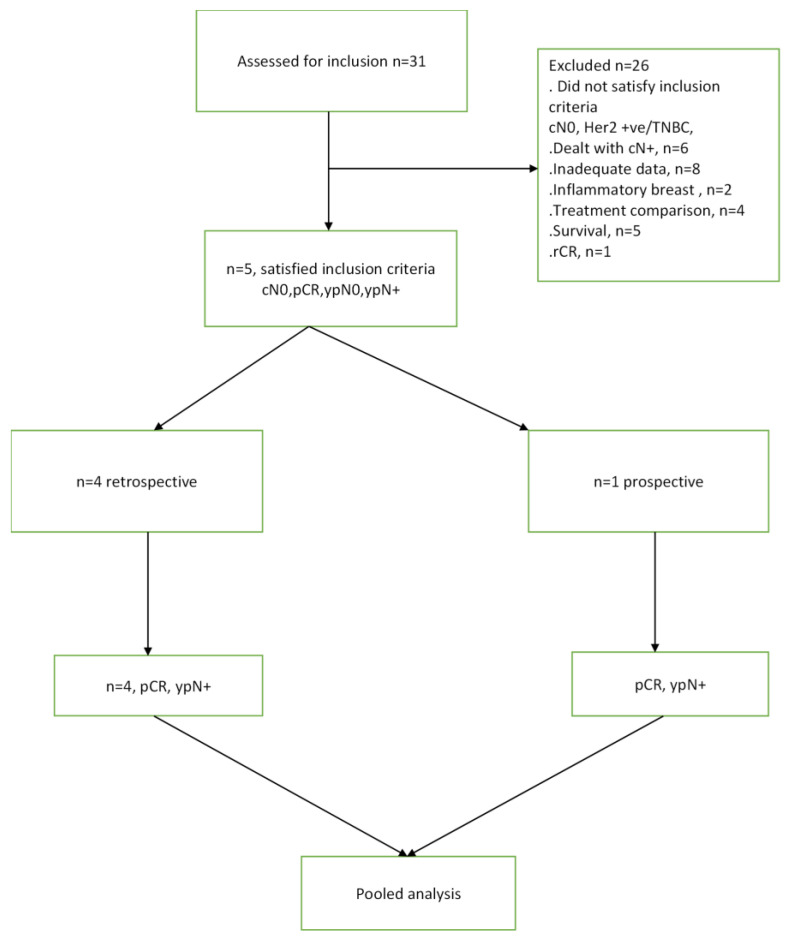
Recent advances in systemic treatment for breast cancer have been underpinned by recognising and exploiting subtype-specific vulnerabilities to achieve higher rates of pathologic complete response (pCR) after neo-adjuvant systemic therapy (NAST). This down-staging of disease has permitted safe surgical de-escalation in patients who respond well. Triple-negative (TNBC) or HER2-positive breast cancer is most likely to achieve complete radiological response (rCR) and pCR after NAST. Hence, for selected patients, particularly those who are clinically node-negative (cN0) at diagnosis, the probability of disease in the sentinel node after NAST could be low enough to justify omitting axillary surgery. The aim of this pooled analysis was to determine the rate of sentinel node positivity (ypN+) in patients with TNBC or HER2-positive breast cancer who were initially cN0, achieving rCR and/or pCR in the breast after NAST. MedLine was searched using appropriate search terms. Five studies (N = 3834) were included in the pooled analysis, yielding a pooled ypN+ rate of 2.16% (95% CI: 1.70-2.63). This is significantly lower than the acceptable false negative rate of sentinel lymph node biopsy (SLNB) and supports consideration of omission of SLNB in this subset of patients.
Keywords: breast cancer; clinically node negative; complete pathological response; complete radiological response; neoadjuvant systemic chemotherapy; pathological node negative; pathological node positive; sentinel lymph node biopsy.
Conflict of interest statement
Kefah Mokbel has received honoraria for providing academic and clinical advice to Merit Medical. The other authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Brackstone M., Baldassarre F.G., Perera F.E., Cil T., Chavez Mac Gregor M., Dayes I.S., Engel J., Horton J.K., King T.A., Kornecki A., et al. Management of the Axilla in Early-Stage Breast Cancer: Ontario Health (Cancer Care Ontario) and ASCO Guideline. J. Clin. Oncol. 2021;39:3056–3082. doi: 10.1200/JCO.21.00934. - DOI - PubMed
-
- Hughes K.S., Schnaper L.A., Bellon J.R., Cirrincione C.T., Berry D.A., McCormick B., Muss H.B., Smith B.L., Hudis C.A., Winer E.P., et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: Long-term follow-up of CALGB 9343. J. Clin. Oncol. 2013;31:2382–2387. doi: 10.1200/JCO.2012.45.2615. - DOI - PMC - PubMed
-
- Reimer T., Stachs A., Veselinovic K., Polata S., Muller T., Kuhn T., Heil J., Ataseven B., Reitsamer R., Hildebrandt G., et al. Patient-reported outcomes for the Intergroup Sentinel Mamma study (INSEMA): A randomised trial with persistent impact of axillary surgery on arm and breast symptoms in patients with early breast cancer. EClinicalMedicine. 2023;55:101756. doi: 10.1016/j.eclinm.2022.101756. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
