

AI-Based Glioma Grading for a Trustworthy Diagnosis: An Analytical Pipeline for Improved Reliability
- PMID: 37444479
- PMCID: PMC10341156
- DOI: 10.3390/cancers15133369
AI-Based Glioma Grading for a Trustworthy Diagnosis: An Analytical Pipeline for Improved Reliability
Abstract
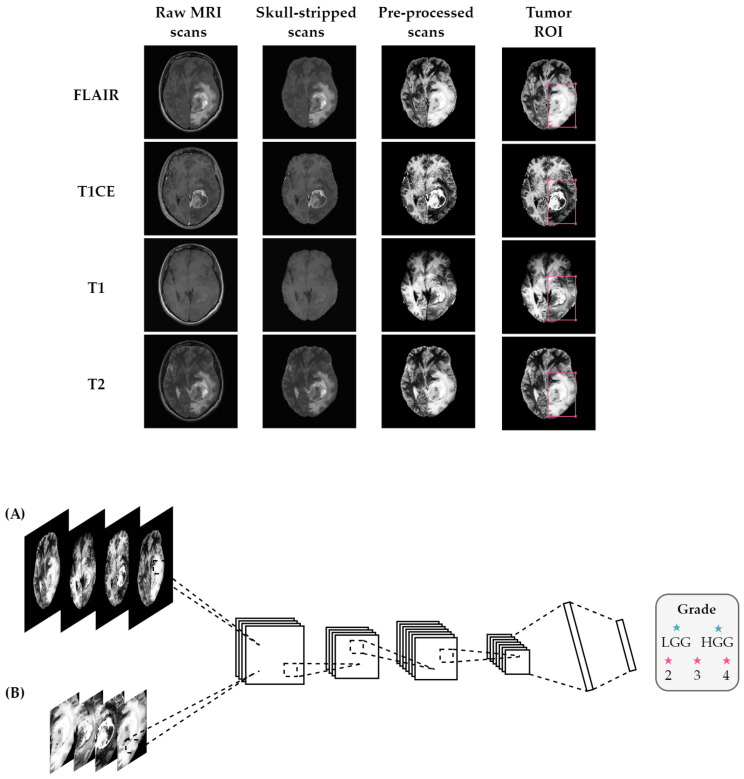
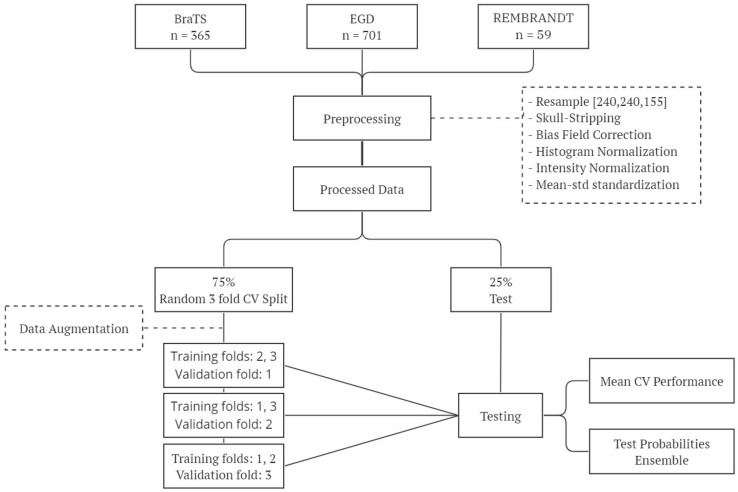
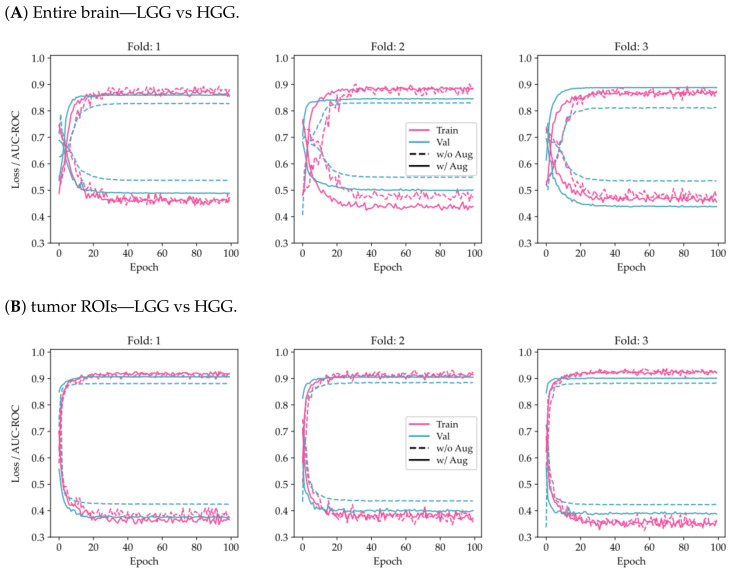
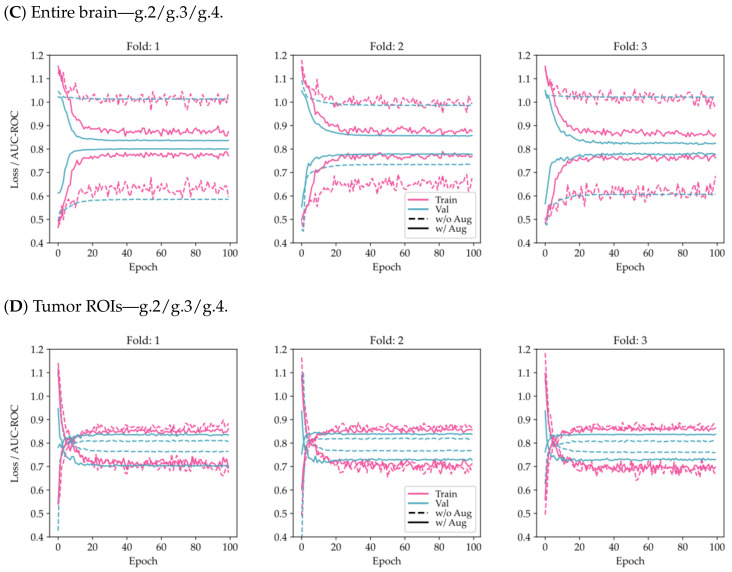
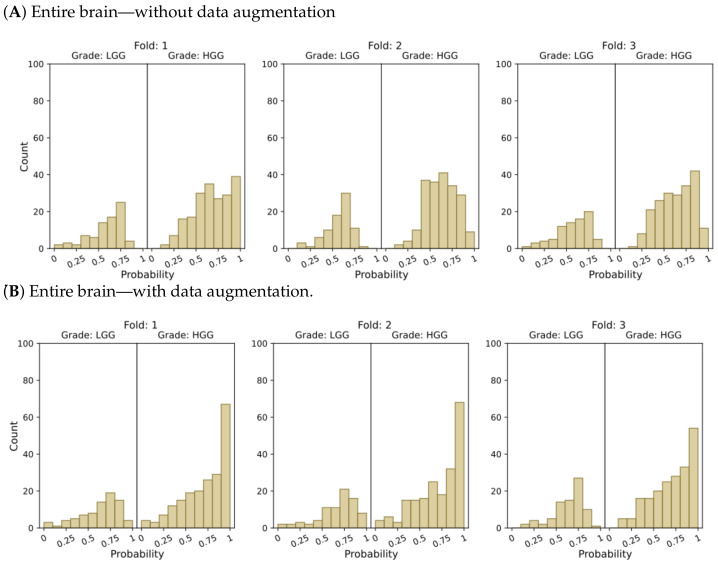
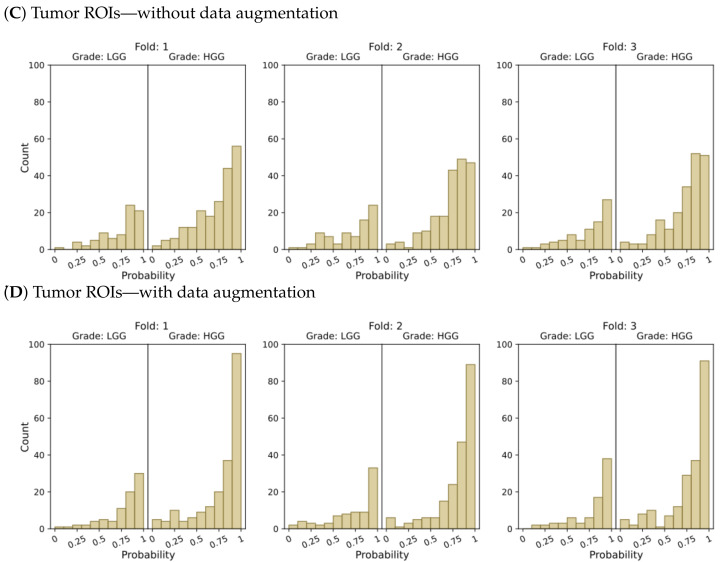
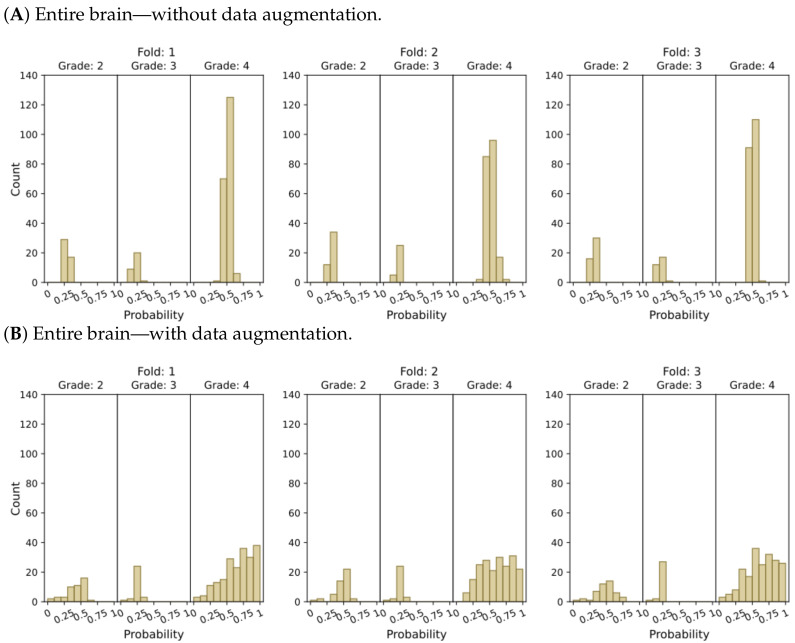
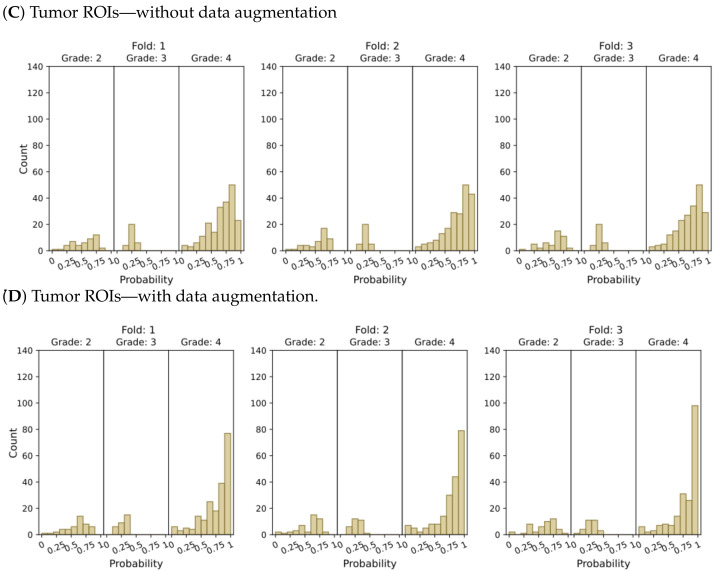
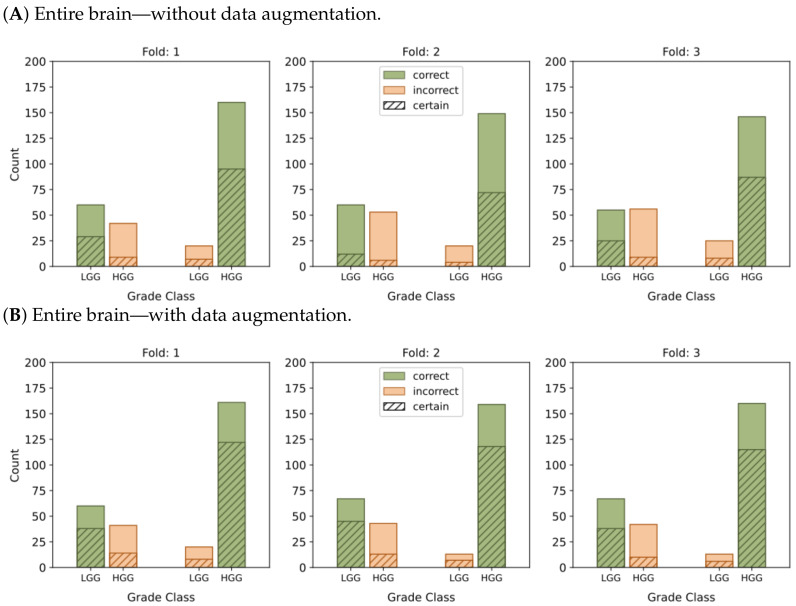
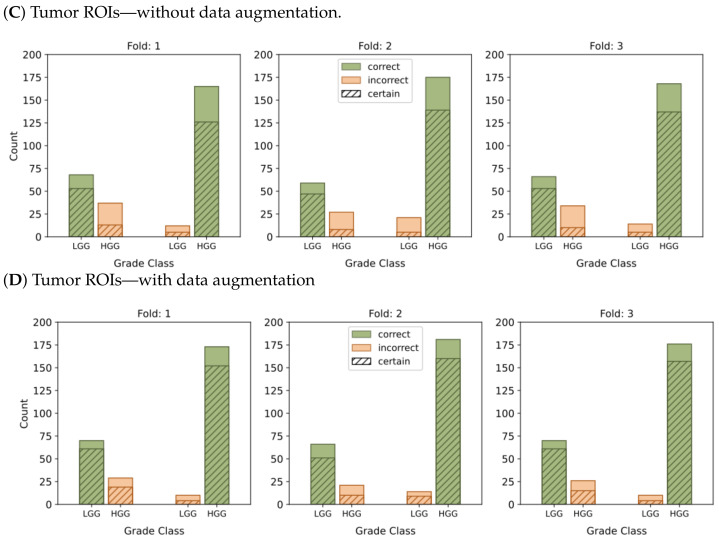
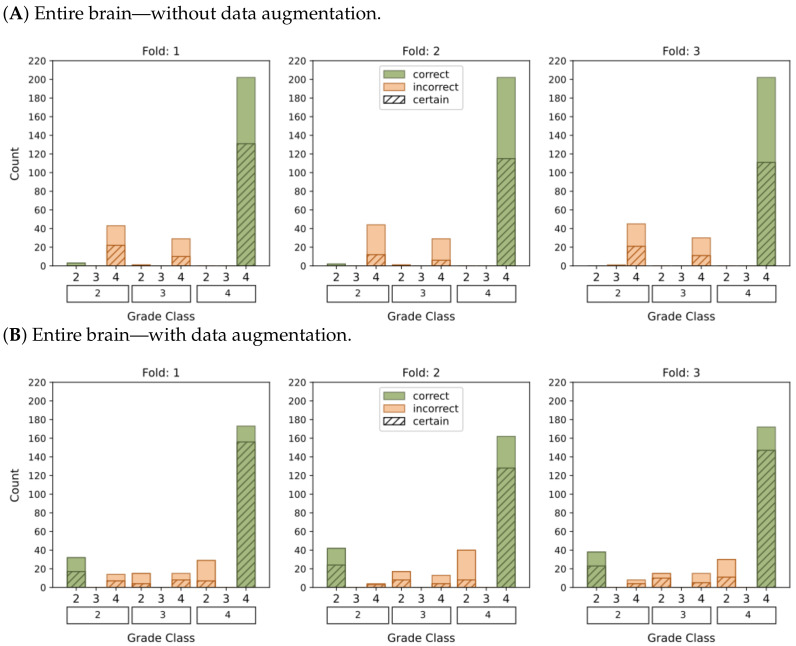
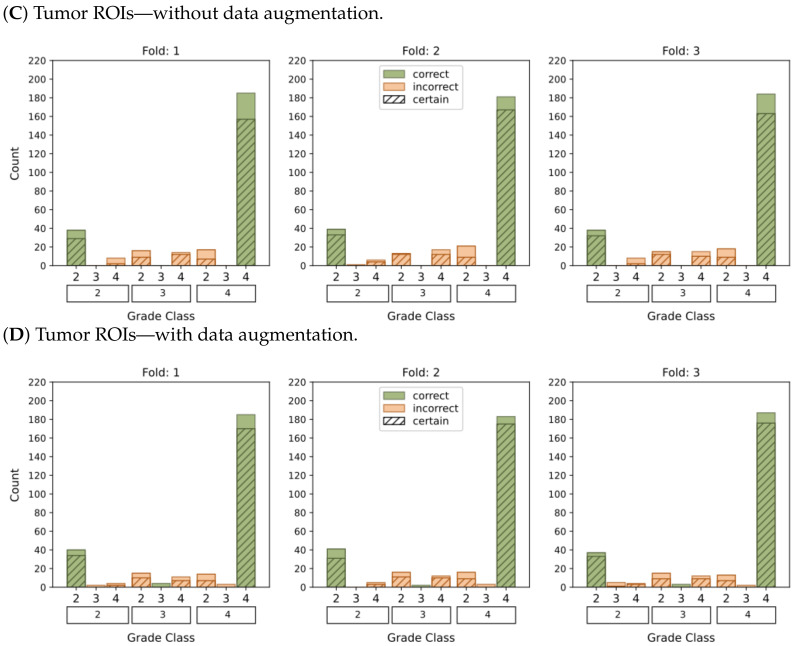
Glioma is the most common type of tumor in humans originating in the brain. According to the World Health Organization, gliomas can be graded on a four-stage scale, ranging from the most benign to the most malignant. The grading of these tumors from image information is a far from trivial task for radiologists and one in which they could be assisted by machine-learning-based decision support. However, the machine learning analytical pipeline is also fraught with perils stemming from different sources, such as inadvertent data leakage, adequacy of 2D image sampling, or classifier assessment biases. In this paper, we analyze a glioma database sourced from multiple datasets using a simple classifier, aiming to obtain a reliable tumor grading and, on the way, we provide a few guidelines to ensure such reliability. Our results reveal that by focusing on the tumor region of interest and using data augmentation techniques we significantly enhanced the accuracy and confidence in tumor classifications. Evaluation on an independent test set resulted in an AUC-ROC of 0.932 in the discrimination of low-grade gliomas from high-grade gliomas, and an AUC-ROC of 0.893 in the classification of grades 2, 3, and 4. The study also highlights the importance of providing, beyond generic classification performance, measures of how reliable and trustworthy the model's output is, thus assessing the model's certainty and robustness.
Keywords: decision support; glioma; machine learning; model certainty; model robustness; neuro-oncology; radiology; reliability; trustworthiness; tumor grading.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Salehiniya H., Farmanfarma K.K. Brain cancer in the world: An epidemiological review. World Cancer Res. J. 2019;6:e1356. doi: 10.32113/wcrj_20197_1356. - DOI
-
- Global Cancer Observatory. [(accessed on 18 April 2023)]. Available online: https://gco.iarc.fr/
-
- Brain Tumours|Cancer Research, UK. [(accessed on 18 April 2023)]. Available online: https://www.cancerresearchuk.org/about-cancer/brain-tumours.
-
- Risk Factors for Brain and Spinal Cord Tumors. [(accessed on 18 April 2023)]. Available online: https://www.cancer.org/cancer/brain-spinal-cord-tumors-adults/causes-ris....
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
