

Dose-Volume Histogram Parameters and Quality of Life in Patients with Prostate Cancer Treated with Surgery and High-Dose Volumetric-Intensity-Modulated Arc Therapy to the Prostate Bed
- PMID: 37444564
- PMCID: PMC10340614
- DOI: 10.3390/cancers15133454
Dose-Volume Histogram Parameters and Quality of Life in Patients with Prostate Cancer Treated with Surgery and High-Dose Volumetric-Intensity-Modulated Arc Therapy to the Prostate Bed
Abstract
Introduction: Prostate bed radiotherapy (RT) is a major affecter of patients' long-term quality of life (QoL). To ensure the best possible outcome of these patients, dose constraints are key for optimal RT planning and delivery. However, establishing refined dose constraints requires access to patient-level data. Therefore, we aimed to provide such data on the relationship between OAR and gastrointestinal (GI) as well as genitourinary (GU) QoL outcomes of a homogenous patient cohort who received dose-intensified post-operative RT to the prostate bed. Furthermore, we aimed to conduct an exploratory analysis of the resulting data.
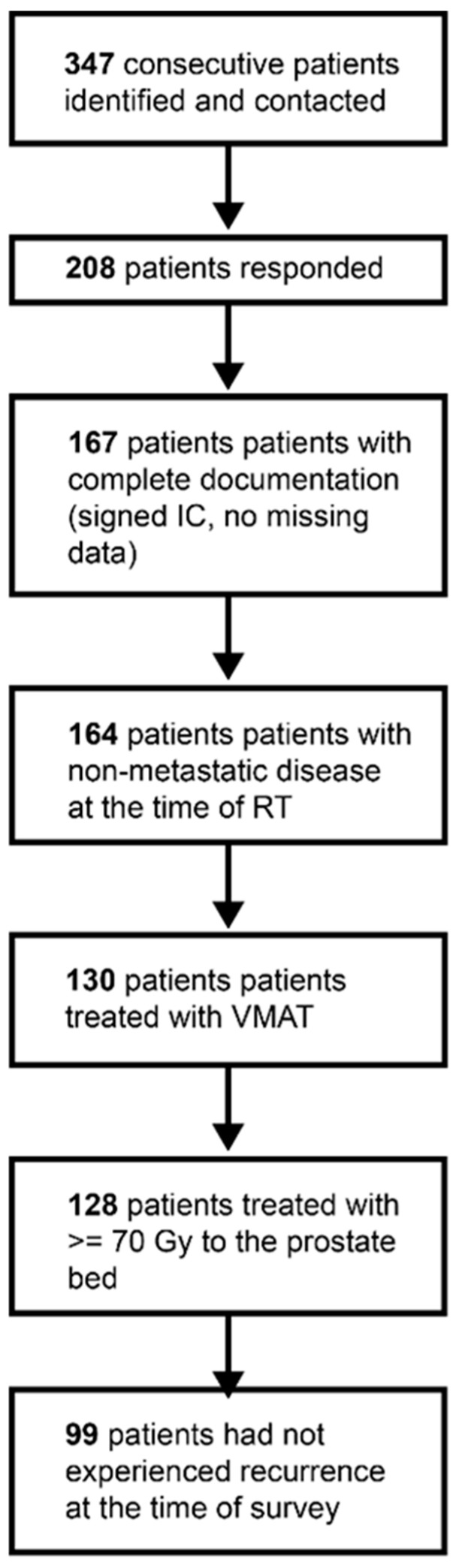
Methods: Patients who were treated with prostate bed RT between 2010 and 2020 were inquired about their QoL based on the Expanded Prostate Cancer Index Composite (EPIC). Those (n = 99) who received volumetric arc therapy (VMAT) of at least 70 Gy to the prostate bed were included. Dose-volume histogram (DVH) parameters were gathered and correlated with the EPIC scores.
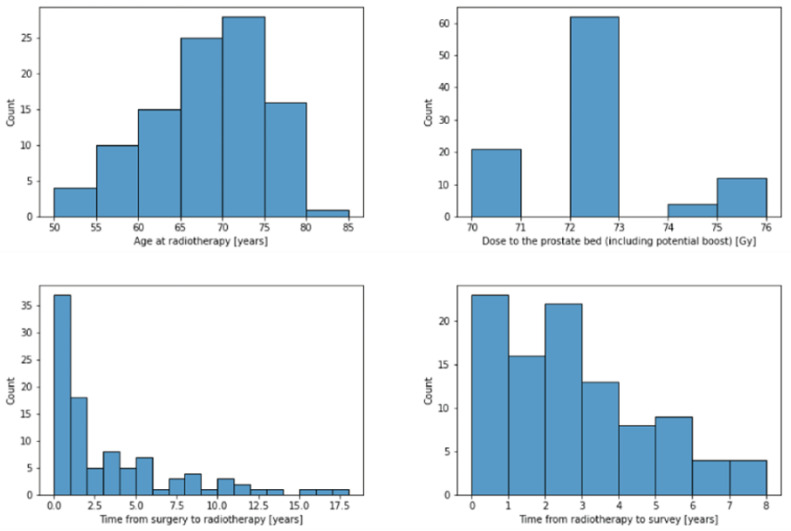
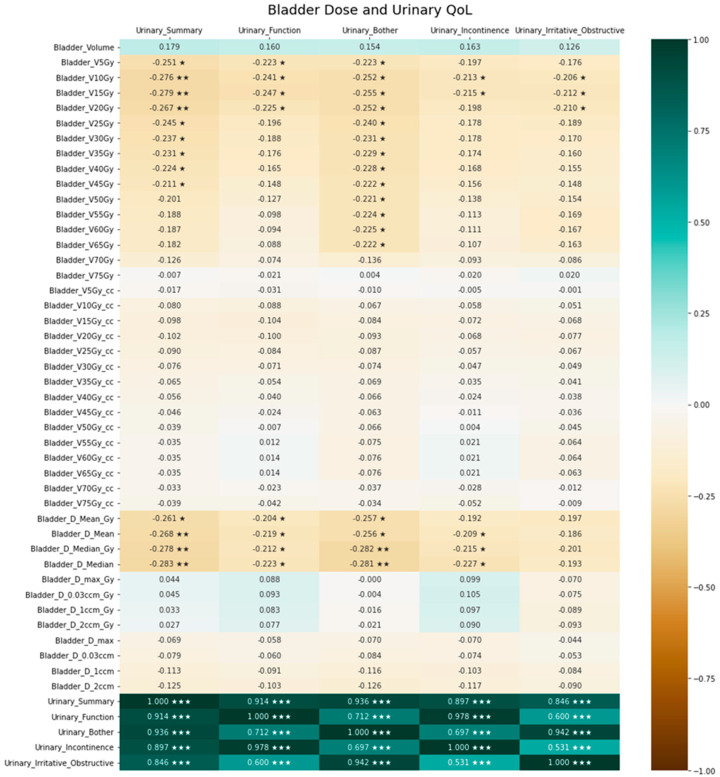
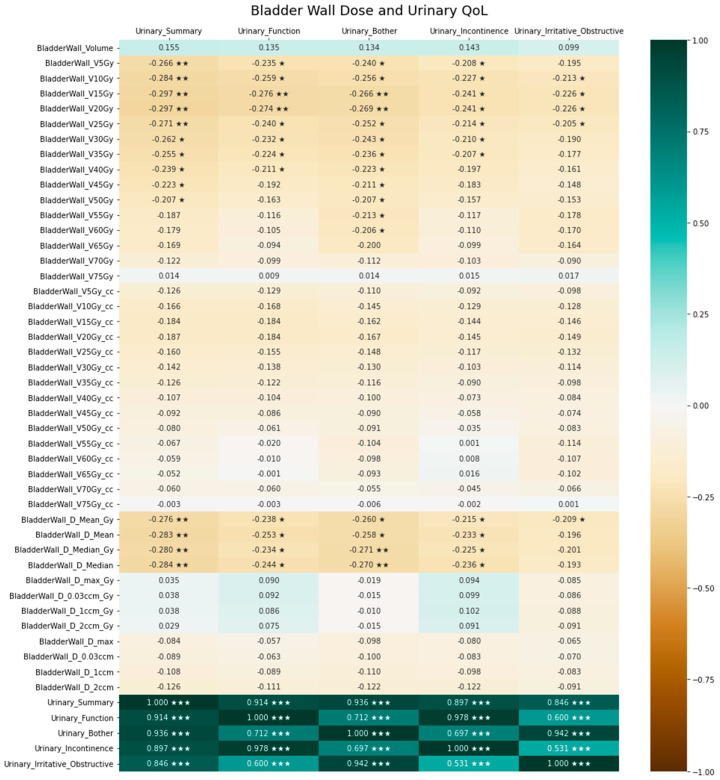
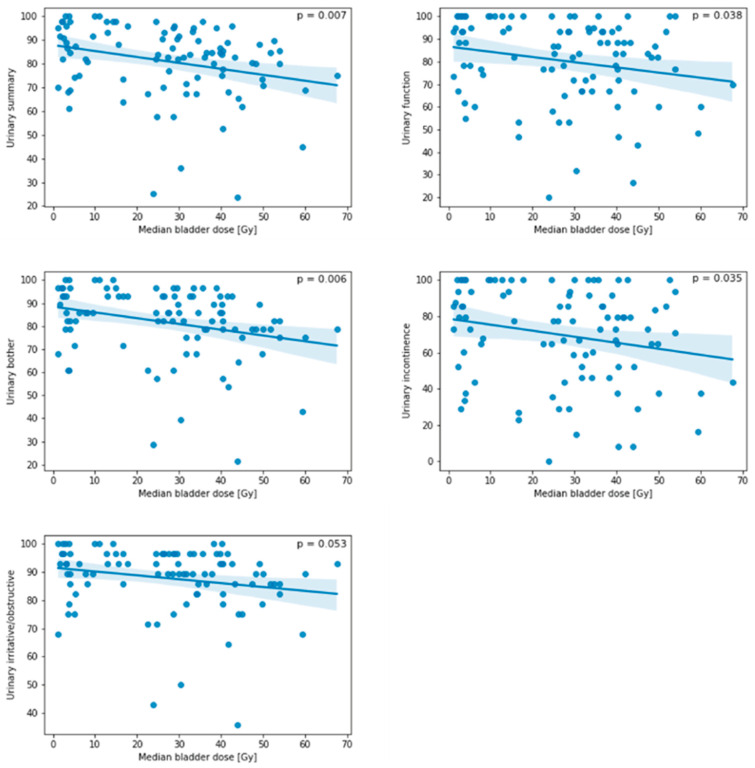
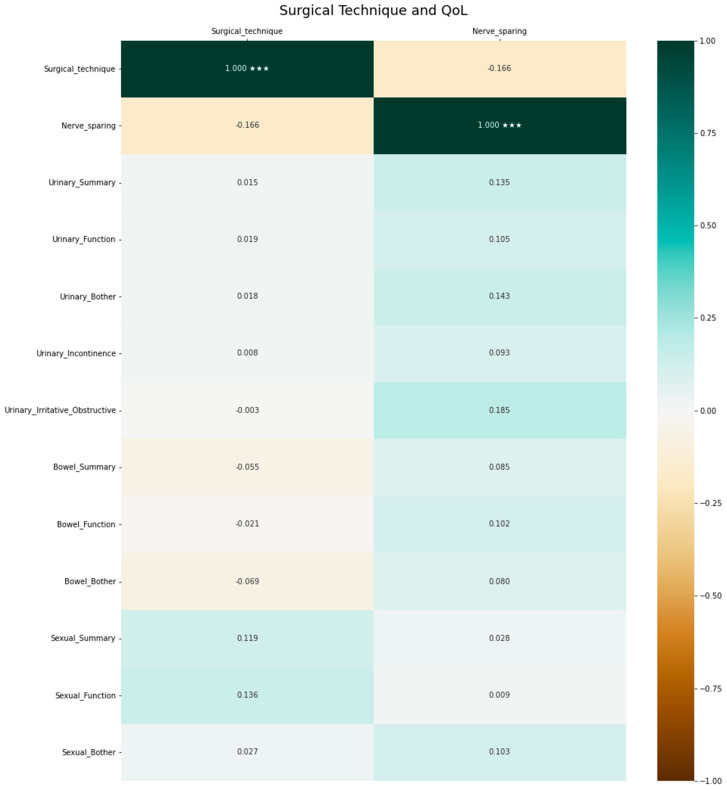
Results: The median age at the time of prostate bed RT was 68.9 years, and patients were inquired about their QoL in the median 2.3 years after RT. The median pre-RT prostate-specific antigen (PSA) serum level was 0.35 ng/mL. The median duration between surgery and RT was 1.5 years. The median prescribed dose to the prostate bed was 72 Gy. A total of 61.6% received prostate bed RT only. For the bladder, the highest level of statistical correlation (p < 0.01) was seen for V10-20Gy, Dmean and Dmedian with urinary QoL. For bladder wall, the highest level of statistically significant correlation (p < 0.01) was seen for V5-25Gy, Dmean and Dmedian with urinary QoL. Penile bulb V70Gy was statistically significantly correlated with sexual QoL (p < 0.05). A larger rectal volume was significantly correlated with improved bowel QoL (p < 0.05). Sigmoid and urethral DVH parameters as well as the surgical approach were not statistically significantly correlated with QoL.
Conclusion: Specific dose constraints for bladder volumes receiving low doses seem desirable for the further optimization of prostate bed RT. This may be particularly relevant in the context of the aspiration of establishing focal RT of prostate cancer and its local recurrences. Our comprehensive dataset may aid future researchers in achieving these goals.
Keywords: dose constraints; dose-volume histogram; prostate bed; prostate cancer; quality of life; radiotherapy.
Conflict of interest statement
P.W. has a patent application titled ‘Method for detection of neurological abnormalities’ outside of the submitted work. The remaining authors declare no conflict of interest.
Figures
References
-
- Bentzen S.M., Constine L.S., Deasy J.O., Eisbruch A., Jackson A., Marks L.B., Ten Haken R.K., Yorke E.D. Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC): An Introduction to the Scientific Issues. Int. J. Radiat. Oncol. Biol. Phys. 2010;76:S3–S9. doi: 10.1016/j.ijrobp.2009.09.040. - DOI - PMC - PubMed
-
- Petersen P.M., Cook A.D., Sydes M.R., Clarke N., Cross W., Kynaston H., Logue J., Neville P., Payne H., Parmar M.K., et al. Salvage Radiation Therapy after Radical Prostatectomy: Analysis of Toxicity by Dose-Fractionation in the RADICALS-RT Trial. Int. J. Radiat. Oncol. Biol. Phys. 2023 doi: 10.1016/j.ijrobp.2023.04.032. - DOI - PMC - PubMed
-
- Kneebone A., Fraser-Browne C., Duchesne G.M., Fisher R., Frydenberg M., Herschtal A., Williams S.G., Brown C., Delprado W., Haworth A., et al. Adjuvant Radiotherapy versus Early Salvage Radiotherapy Following Radical Prostatectomy (TROG 08.03/ANZUP RAVES): A Randomised, Controlled, Phase 3, Non-Inferiority Trial. Lancet Oncol. 2020;21:1331–1340. doi: 10.1016/S1470-2045(20)30456-3. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
