

Stair-Climbing Tests or Self-Reported Functional Capacity for Preoperative Pulmonary Risk Assessment in Patients with Known or Suspected COPD-A Prospective Observational Study
- PMID: 37445215
- PMCID: PMC10342346
- DOI: 10.3390/jcm12134180
Stair-Climbing Tests or Self-Reported Functional Capacity for Preoperative Pulmonary Risk Assessment in Patients with Known or Suspected COPD-A Prospective Observational Study
Abstract
Background: This prospective study aims to determine whether preoperative stair-climbing tests (SCT) predict postoperative pulmonary complications (PPC) better than self-reported poor functional capacity (SRPFC) in patients with known or suspected COPD.
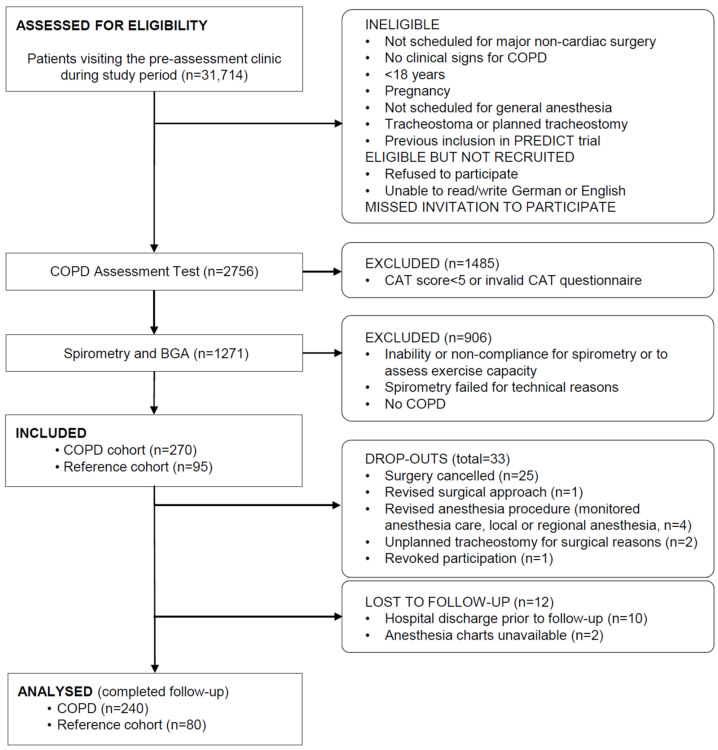
Methods: A total of 320 patients undergoing scheduled for major non-cardiac surgery, 240 with verified COPD and 80 with GOLD key indicators but disproved COPD, underwent preoperative SRPFC and SCT and were analyzed. Least absolute shrinkage and selection operator (LASSO) regression was used for variable selection. Two multivariable regression models were fitted, the SRPFC model (baseline variables such as sociodemographic, surgical and procedural characteristics, medical preconditions, and GOLD key indicators plus SRPFC) and the SCT model (baseline variables plus SCTPFC).
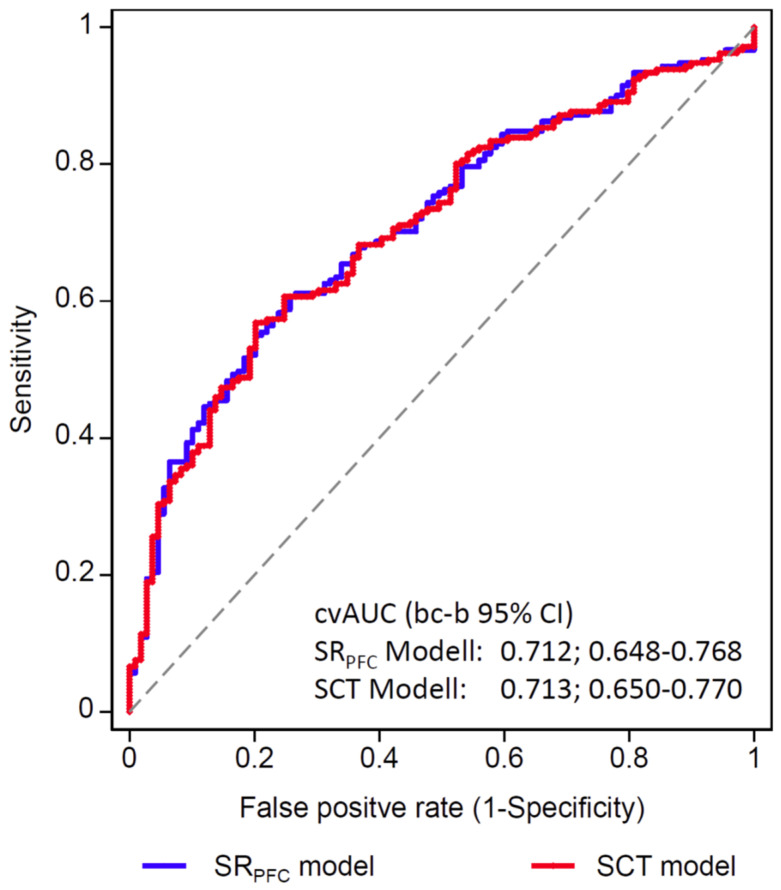
Results: Within all stair-climbing variables, LASSO exclusively selected self-reported poor functional capacity. The cross-validated area under the receiver operating characteristic curve with bias-corrected bootstrapping 95% confidence interval (95% CI) did not differ between the SRPFC and SCT models (0.71; 0.65-0.77 for both models). SRPFC was an independent risk factor (adjusted odds ratio (OR) 5.45; 95% CI 1.04-28.60; p = 0.045 in the SRPFC model) but SCTPFC was not (adjusted OR 3.78; 95% CI 0.87-16.34; p = 0.075 in the SCT model).
Conclusions: Our findings indicate that preoperative SRPFC adequately predicts PPC while additional preoperative SCTs are dispensable in patients with known or suspected COPD.
Keywords: chronic obstructive pulmonary disease; postoperative pulmonary complication; preoperative; pulmonary risk; self-reported poor functional capacity; stair-climbing test.
Conflict of interest statement
M.P. is a member of the Medical Advisory Board of Radiometer Medical, Copenhagen, Denmark. M.P. received a research grant awarded by Verathon Inc., Bothell, WA, USA. The other authors declare no competing interests.
Figures
Similar articles
-
Preoperative Spirometry in Patients With Known or Suspected Chronic Obstructive Pulmonary Disease Undergoing Major Surgery: The Prospective Observational PREDICT Study.Anesth Analg. 2023 Oct 1;137(4):806-818. doi: 10.1213/ANE.0000000000006235. Epub 2022 Nov 1. Anesth Analg. 2023. PMID: 36730893
-
Association between recovery from desaturation after stair climbing and postoperative complications in lung resection.Gen Thorac Cardiovasc Surg. 2025 Mar;73(3):171-179. doi: 10.1007/s11748-024-02059-1. Epub 2024 Jul 15. Gen Thorac Cardiovasc Surg. 2025. PMID: 39008147
-
Gait Analysis Reveals that Total Hip Arthroplasty Increases Power Production in the Hip During Level Walking and Stair Climbing.Clin Orthop Relat Res. 2019 Aug;477(8):1839-1847. doi: 10.1097/CORR.0000000000000809. Clin Orthop Relat Res. 2019. PMID: 31135537 Free PMC article.
-
Performance at stair-climbing test is associated with postoperative complications after lung resection: a systematic review and meta-analysis.Thorax. 2020 Sep;75(9):791-797. doi: 10.1136/thoraxjnl-2019-214019. Epub 2020 Jul 10. Thorax. 2020. PMID: 32651199 Free PMC article.
-
Stem cell therapy for dilated cardiomyopathy.Cochrane Database Syst Rev. 2021 Jul 21;7(7):CD013433. doi: 10.1002/14651858.CD013433.pub2. Cochrane Database Syst Rev. 2021. PMID: 34286511 Free PMC article.
References
-
- Fleisher L.A., Fleischmann K.E., Auerbach A.D., Barnason S.A., Beckman J.A., Bozkurt B., Davila-Roman V.G., Gerhard-Herman M.D., Holly T.A., Kane G.C., et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:2215–2245. doi: 10.1161/CIR.0000000000000105. - DOI - PubMed
-
- Halvorsen S., Mehilli J., Cassese S., Hall T.S., Abdelhamid M., Barbato E., De Hert S., de Laval I., Geisler T., Hinterbuchner L., et al. 2022 ESC Guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery. Eur. Heart J. 2022;43:3826–3924. doi: 10.1093/eurheartj/ehac270. - DOI - PubMed
-
- Wijeysundera D.N., Beattie W.S., Hillis G.S., Abbott T.E.F., Shulman M.A., Ackland G.L., Mazer C.D., Myles P.S., Pearse R.M., Cuthbertson B.H., et al. Integration of the Duke Activity Status Index into preoperative risk evaluation: A multicentre prospective cohort study. Br. J. Anaesth. 2020;124:261–270. doi: 10.1016/j.bja.2019.11.025. - DOI - PubMed
-
- Wijeysundera D.N., Pearse R.M., Shulman M.A., Abbott T.E.F., Torres E., Ambosta A., Croal B.L., Granton J.T., Thorpe K.E., Grocott M.P.W., et al. Assessment of functional capacity before major non-cardiac surgery: An international, prospective cohort study. Lancet. 2018;391:2631–2640. doi: 10.1016/S0140-6736(18)31131-0. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
