

Associations of Traditionally Determined Left Ventricular Mass Indices and Hemodynamic and Non-Hemodynamic Components of Cardiac Remodeling with Diastolic and Systolic Function in Patients with Chronic Kidney Disease
- PMID: 37445246
- PMCID: PMC10342723
- DOI: 10.3390/jcm12134211
Associations of Traditionally Determined Left Ventricular Mass Indices and Hemodynamic and Non-Hemodynamic Components of Cardiac Remodeling with Diastolic and Systolic Function in Patients with Chronic Kidney Disease
Abstract
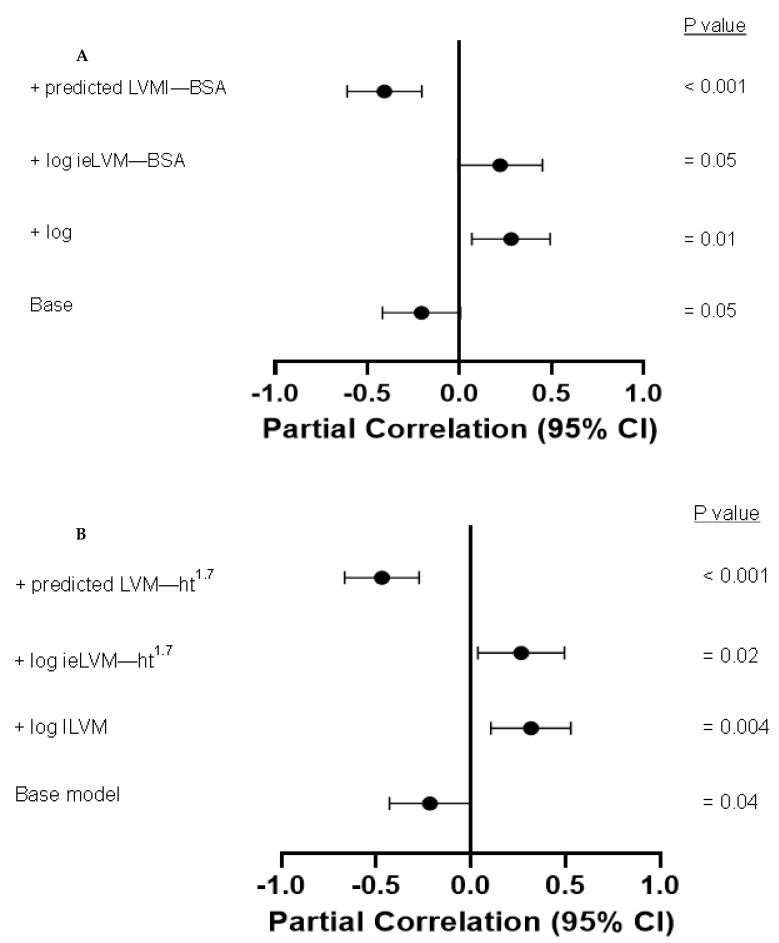
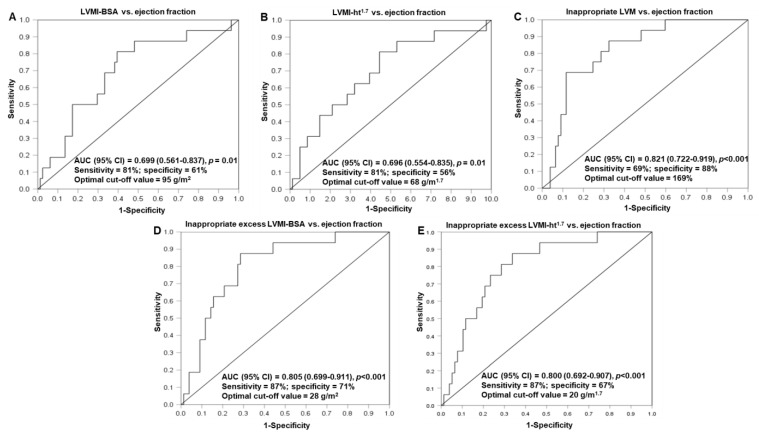
We aimed to evaluate the extent to which different left ventricular mass parameters are associated with left ventricular function in chronic kidney disease (CKD) patients. We compared the associations between traditionally determined left ventricular mass indices (LVMIs) and hemodynamic (predicted LVMIs) and non-hemodynamic remodeling parameters with left ventricular function in patients with CKD; non-hemodynamic remodeling was represented by inappropriate left ventricular mass and inappropriate excess LVMIs (traditionally determined LVMIs-predicted LVMIs). Non-hemodynamic left ventricular remodeling parameters were strongly associated with impaired left ventricular systolic function (p < 0.001), whereas hemodynamic left ventricular remodeling was also related strongly (p < 0.001) but directly to left ventricular systolic function. Independent of one another, hemodynamic and non-hemodynamic left ventricular remodeling had associations in opposite directions to left ventricular systolic function and was associated directly with traditionally determined left ventricular mas indices (p < 0.001 for all relationships). Non-hemodynamic cardiac remodeling parameters discriminated more effectively than traditionally determined LVMIs between patients with and without reduced ejection fraction (p < 0.04 for comparison). Left ventricular mass parameters were unrelated to impaired diastolic function in patients with CKD. Traditionally determined LVMIs are less strongly associated with impaired systolic function than non-hemodynamic remodeling parameters (p < 0.04-0.01 for comparisons) because they represent both adaptive or compensatory and non-hemodynamic cardiac remodeling.
Keywords: chronic kidney disease; diastolic–systolic function; hemodynamic; non-hemodynamic cardiac remodeling components; traditionally determined left ventricular mass index.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hickson L.J., Negrotto S.N., Onuigbo M., Scott C.G., Rule A.D., Norby S.M., Albright R.C., Casey E.T., Dillon J.J., Pellika P.A., et al. Echocardiography Criteria for Structural Heart Disease in Patients with End-Stage Renal Disease Initiating Haemodialysis. J. Am. Coll. Cardiol. 2016;67:1173–1182. doi: 10.1016/j.jacc.2015.12.052. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
