

Persistent Increase in Serum Ferritin Levels despite Converting to Permanent Vascular Access in Pediatric Hemodialysis Patients: Pediatric Nephrology Research Consortium Study
- PMID: 37445286
- PMCID: PMC10342380
- DOI: 10.3390/jcm12134251
Persistent Increase in Serum Ferritin Levels despite Converting to Permanent Vascular Access in Pediatric Hemodialysis Patients: Pediatric Nephrology Research Consortium Study
Abstract
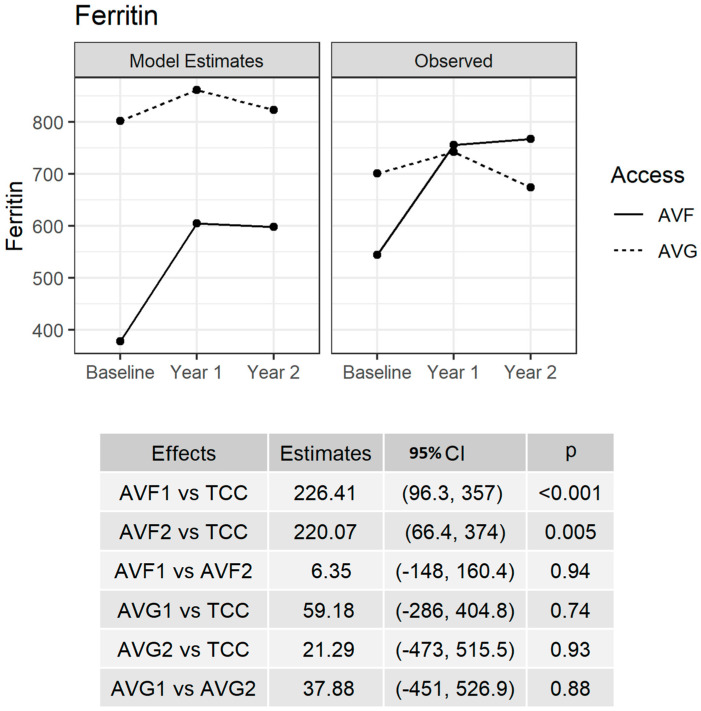
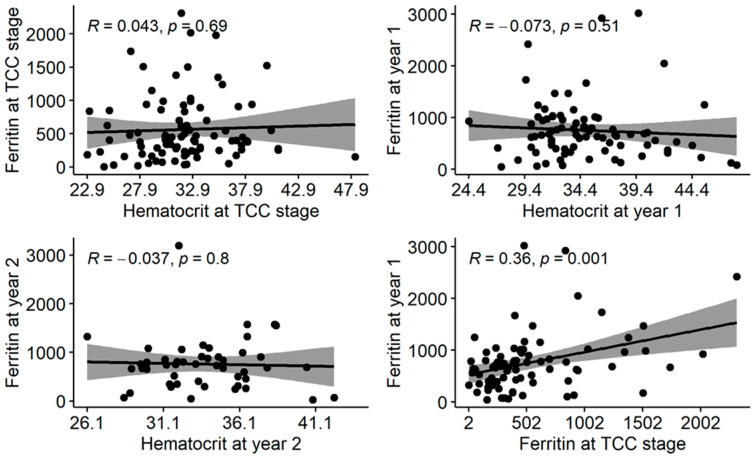
Our objective was to examine serum ferritin trends after conversion to permanent vascular access (PVA) among children who started hemodialysis (HD) using tunneled cuffed catheters (TCC). Retrospective chart reviews were completed on 98 subjects from 20 pediatric HD centers. Serum ferritin levels were collected at the creation of PVA and for two years thereafter. There were 11 (11%) arteriovenous grafts (AVG) and 87 (89%) arteriovenous fistulae (AVF). Their mean TCC use was 10.4 ± 17.3 months. Serum ferritin at PVA creation was elevated at 562.64 ± 492.34 ng/mL, increased to 753.84 ± 561.54 ng/mL (p = < 0.001) in the first year and remained at 759.60 ± 528.11 ng/mL in the second year (p = 0.004). The serum ferritin levels did not show a statistically significant linear association with respective serum hematocrit values. In a multiple linear regression model, there were three predictors of serum ferritin during the first year of follow-up: steroid-resistant nephrotic syndrome as primary etiology (p = 0.035), being from a center that enrolled >10 cases (p = 0.049) and baseline serum ferritin level (p = 0.017). Increasing serum ferritin after conversion to PVA is concerning. This increase is not associated with serum hematocrit trends. Future studies should investigate the correlation of serum transferrin saturation and ferritin levels in pediatric HD patients.
Keywords: arteriovenous fistula; arteriovenous graft; ferritin; hemodialysis; pediatric.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Conversion to permanent vascular access is associated with improved markers of hemodialysis efficacy in children: Pediatric nephrology research consortium study.Clin Nephrol. 2021 Nov;96(5):270-280. doi: 10.5414/CN110455. Clin Nephrol. 2021. PMID: 34190683
-
Predictors of time to first cannulation for arteriovenous fistula in pediatric hemodialysis patients: Midwest Pediatric Nephrology Consortium study.Pediatr Nephrol. 2020 Feb;35(2):287-295. doi: 10.1007/s00467-019-04396-3. Epub 2019 Nov 6. Pediatr Nephrol. 2020. PMID: 31696356
-
Predictors of patency for arteriovenous fistulae and grafts in pediatric hemodialysis patients.Pediatr Nephrol. 2019 Feb;34(2):329-339. doi: 10.1007/s00467-018-4082-4. Epub 2018 Sep 27. Pediatr Nephrol. 2019. PMID: 30264215
-
Gender differences in vascular access in hemodialysis patients in the United States: developing strategies for improving access outcome.Gend Med. 2007 Sep;4(3):193-204. doi: 10.1016/s1550-8579(07)80040-4. Gend Med. 2007. PMID: 18022587 Review.
-
Surgical creation of upper extremity arteriovenous fistula and grafts: a narrative review.Cardiovasc Diagn Ther. 2023 Feb 28;13(1):147-155. doi: 10.21037/cdt-21-565. Epub 2022 Jul 19. Cardiovasc Diagn Ther. 2023. PMID: 36864949 Free PMC article. Review.
Cited by
-
Analysis of arteriovenous fistula failure factors and construction of nomogram prediction model in patients with maintenance hemodialysis.Ren Fail. 2025 Dec;47(1):2500665. doi: 10.1080/0886022X.2025.2500665. Epub 2025 Jun 1. Ren Fail. 2025. PMID: 40451732 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
