

Allogenic Cancellous Bone versus Injectable Bone Substitute for Endoscopic Treatment of Simple Bone Cyst and Intraosseous Lipoma of the Calcaneus and Is Intraosseous Lipoma a Developmental Stage of a Simple Bone Cyst?
- PMID: 37445307
- PMCID: PMC10342899
- DOI: 10.3390/jcm12134272
Allogenic Cancellous Bone versus Injectable Bone Substitute for Endoscopic Treatment of Simple Bone Cyst and Intraosseous Lipoma of the Calcaneus and Is Intraosseous Lipoma a Developmental Stage of a Simple Bone Cyst?
Abstract
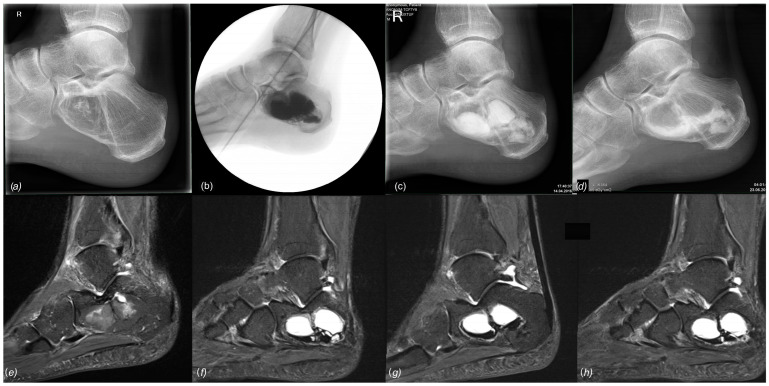
Simple bone cysts (SBCs) and intraosseous lipoma (IOL) of the calcaneus are rare tumor entities that are primarily diagnosed due to unspecific heel pain, incidental findings, or rarely due to pathological fractures. Compared to traditional open tumor resections, endoscopic resection of these benign tumors aims to minimize surgical morbidity and maximize surgical efficiency without compromising safety. Grafting is regularly performed to reduce the risk of recurrence and stimulate osseous consolidation of the lytic lesion. As the incidence is low and treatment strategies are heterogeneous, there is no clear consensus for the treatment of simple cysts or intraosseous lipomas of the calcaneus. The objectives of this study are (a) to present medium to long-term results after endoscopic resection and grafting with allogenic cancellous bone or bioresorbable hydroxyapatite and calcium sulfate cement, and (b) to add further evidence to the discussion of whether calcaneal SBC and IOL are the same entity at different developmental stages. Between 2012 and 2019, a total of 25 benign bone tumors consisting of 17 SBCs and 8 IOLs were treated by A.T. with endoscopic resection and grafting, comprising the largest cohort to date. For grafting, 12 patients received allogenic cancellous bone (group A) and 13 patients received injectable bone substitute (group B). Pre- and postoperative imaging using plain X-rays and MRI was retrospectively analyzed with a mean follow-up time of 24.5 months to assess tumor size, osseous consolidation (modified Neer classification), and tumor recurrence. A retrospective chart analysis focusing on adverse intra- and perioperative events and other complications associated with the surgical procedure was performed using the modified Clavien-Dindo classification (CD1-3). A total of 12/13 cases with allogenic bone grafting showed a Neer Type 1 osseous healing of the tumorous lesion after endoscopic resection, whereas only 5/11 cases with injectable bone substitute showed sufficient healing (types 1 and 2). There were three recurrent cysts (Neer 4) and two persistent cysts (Neer 3) after using injectable bone substitute. Two CD1 complications were observed in group A (prolonged wound drainage, sural neuritis) and eight complications were observed in group B (6× CD1, 2× CD3). At least two IOLs diagnosed preoperatively using MRI were ultimately identified as SBCs upon histopathologic examination. Allogenic cancellous bone grafting after endoscopic resection of calcaneal SBC or IOL showed a very low rate of complications and no tumor recurrence in our series. On the other hand, depending on the material used, injectable bone substitute showed a high rate of "white-out" (excessive drainage), resulting in multiple complications such as prolonged wound healing, insufficient permanent defect filling, recurrence, and revision surgery. Over time, calcaneal SBC may transform into IOL, exhibiting distinct features of both entities simultaneously during ossoscopy and histopathological analysis.
Keywords: allografting; benign bone tumor; calcaneal bone cyst; endoscopy; injectable bone substitute; intra-osseous lipoma; lipoma of bone; ossoscopy; simple bone cyst; white-out.
Conflict of interest statement
The authors declare no conflict of interest.
Figures










References
-
- Reith J., Bloem J., Forsyth R. WHO Classification of Tumours Soft Tissue and Bone Tumours. 5th ed. International Agency for Research on Cancer (IARC) 150 Cours Albert Thomas; Lyon, France: 2020. - DOI
-
- Mirra J. Bone Tumors: Clinical, Rardiologic, and Pathologic Correlations. Philadelphia; London, UK: 1989.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
