

Dynamics of Bone Disease Biomarkers Dickkopf-1 and Sclerostin in Patients with Multiple Myeloma
- PMID: 37445475
- PMCID: PMC10342782
- DOI: 10.3390/jcm12134440
Dynamics of Bone Disease Biomarkers Dickkopf-1 and Sclerostin in Patients with Multiple Myeloma
Abstract
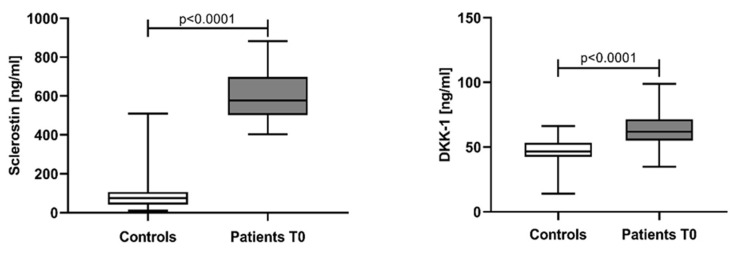
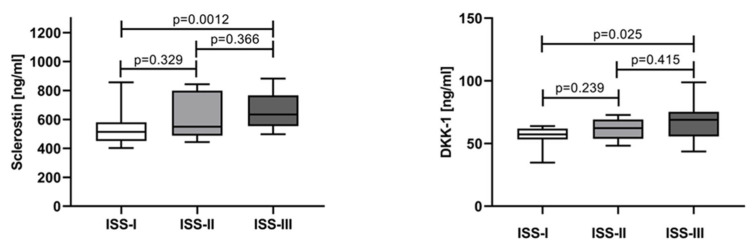
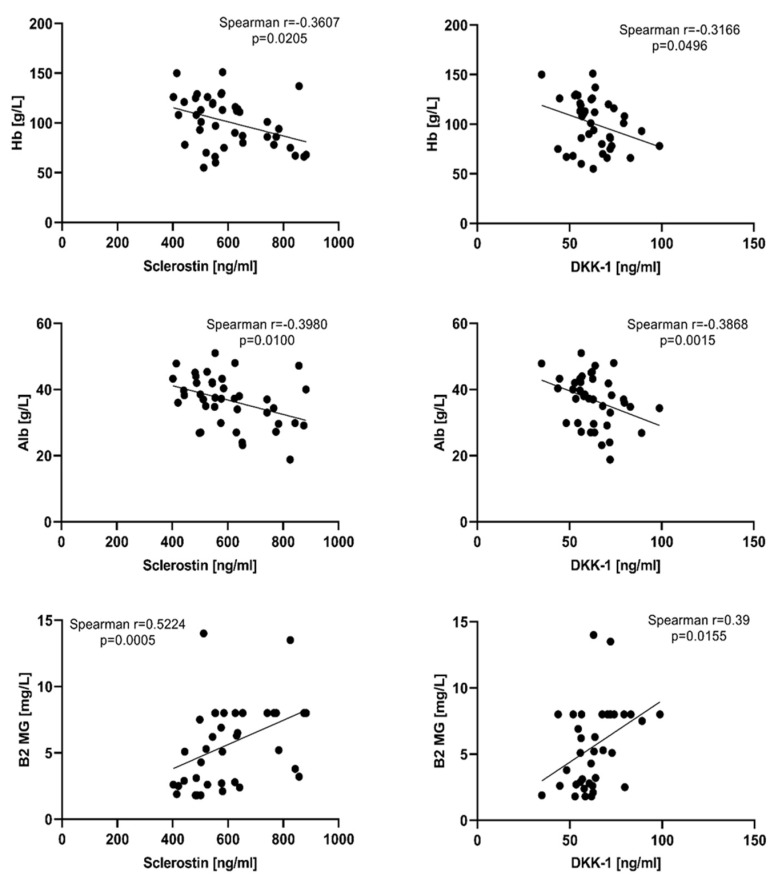
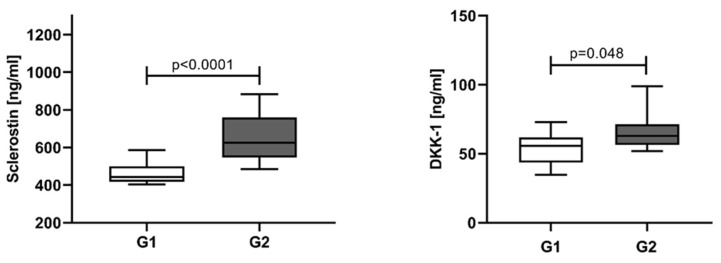
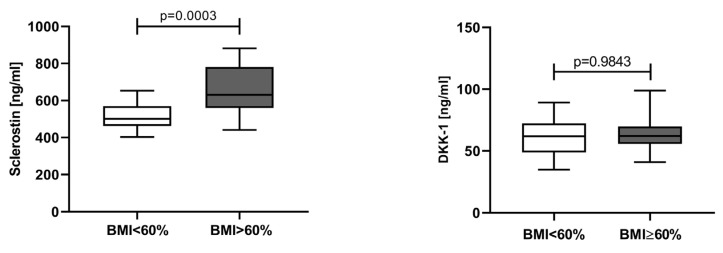
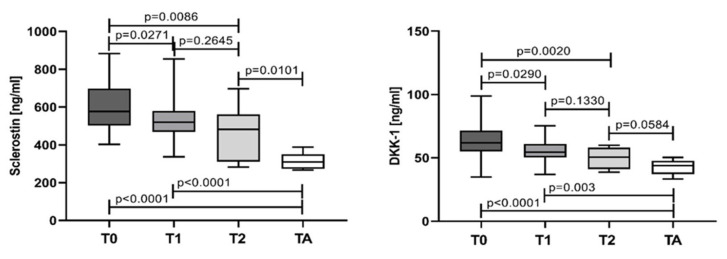
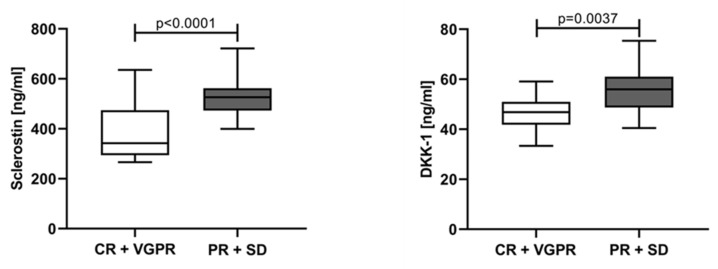
Dickkopf-1 (DKK-1) and sclerostin are essential Wnt/β-catenin pathway inhibitors, playing an important role in multiple myeloma bone disease (MBD). We aimed to examine the serum DKK-1 and sclerostin variations in newly diagnosed multiple myeloma (NDMM) patients at diagnosis and in the course of therapy, including autologous stem cell transplantation (ASCT). This study included 41 NDMM-patients and 33 controls. MBD was assessed by whole-body low-dose computed tomography. DKK-1 and sclerostin were assayed by commercial ELISA kits. At diagnosis, NDMM-patients revealed significantly higher DKK-1 and sclerostin values (p < 0.0001), showing dependence on disease stage (lowest in ISS-I and highest in ISS-III: p < 0.0012 and p < 0.025, respectively, for both proteins). Bone lesions revealed significant positive correlation with both DKK-1 (p < 0.05) and sclerostin (p < 0.0001). In the course of therapy, significant reduction, more prominent after ASCT, was observed for both parameters in each treatment point compared to the baseline (p < 0.0001). Markedly lower sclerostin (p < 0.01) and DKK-1 (p < 0.05) values were observed in patients with complete and very good partial response compared to those with partial response, stable, or progressive disease. Sclerostin and DKK-1 in NDMM patients reflect the MBD severity and the effect of therapy. Both proteins could represent a novel tool for better disease monitoring and effectiveness of therapy.
Keywords: Dickkopf-1; multiple myeloma bone disease; sclerostin.
Conflict of interest statement
The authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Cowan A.J., Allen C., Barac A., Basaleem H., Bensenor I., Curado M.P., Foreman K., Gupta R., Harvey J., Hosgood H.D., et al. Global Burden of Multiple Myeloma: A Systematic Analysis for the Global Burden of Disease Study 2016. JAMA Oncol. 2018;4:1221–1227. doi: 10.1001/jamaoncol.2018.2128. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
