

Intraspinal and Intracranial Neurotuberculosis, Clinical and Imaging Characteristics and Outcomes in Hospitalized Patients: A Cohort Study (2000-2022)
- PMID: 37445568
- PMCID: PMC10342332
- DOI: 10.3390/jcm12134533
Intraspinal and Intracranial Neurotuberculosis, Clinical and Imaging Characteristics and Outcomes in Hospitalized Patients: A Cohort Study (2000-2022)
Abstract
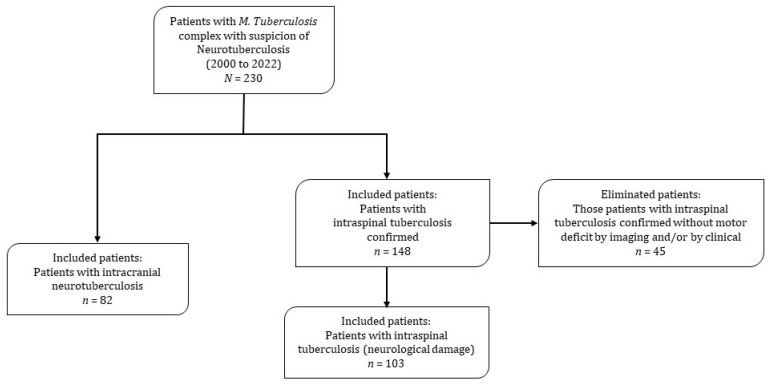
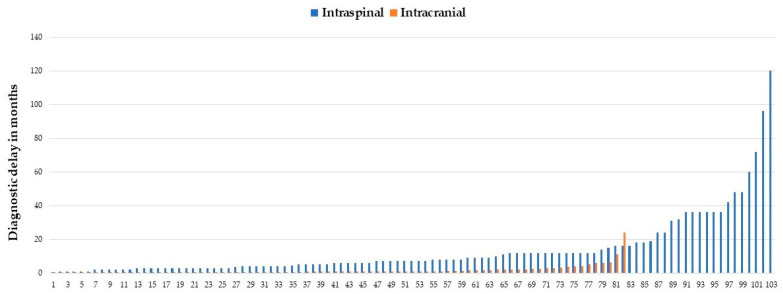
Neurotuberculosis (neuroTB) is a devastating disease, and is difficult to diagnose. The aim of this study was to analyze the clinical and imaging characteristics, and outcomes of a retrospective cohort (2000-2022) of hospitalized patients diagnosed with intraspinal and intracranial neuroTB. This work was designed through clinical, laboratory and imaging findings. Variables included: demographic data, history of tuberculosis, neurological complications, comorbidities and outcomes. Morbi-mortality risk factors were identified by univariate analysis. The cohort included: 103 patients with intraspinal and 82 with intracranial neuroTB. During the study period, in-hospital mortality of 3% for intraspinal and 29.6% for intracranial neuroTB was estimated. Motor deficit was found in all patients with intraspinal neuroTB. Risk factors for the unfavorable outcome of patients with intraspinal neuroTB were: age ≥ 40 years, diabetes mellitus (DM), diagnostic delay, kyphosis and spondylodiscitis ≥ 3 levels of involvement. Among the patients with intracranial neuroTB, 79/82 (96.3%) had meningitis and 22 patients had HIV infection (10 of them died). Risk factors for mortality from intracranial neuroTB were: HIV infection, hydrocephalus, stroke, lymphopenia and disseminated and gastrointestinal TB. Patients with intraspinal neuroTB had a significant number of destroyed vertebrae that determined their neurological deficit status. The mortality burden in intracranial neuroTB was conditioned by HIV infection and renal transplantation patients.
Keywords: clinical characteristics; imaging; intracranial; intraspinal; neurotuberculosis; outcomes.
Conflict of interest statement
The authors declare no conflict of interest and they have read and agreed to the published version of the manuscript.
Figures

References
-
- World Health Organization Tuberculosis Profile: WHO Global. 2021. [(accessed on 28 May 2023)]. Available online: https://worldhealthorg.shinyapps.io/tb_profiles/?_inputs_&lan=%22ES%22&e....
-
- CENAPRECE Casos Nuevos de Tuberculosis Todas Formas Estados Unidos Mexicanos 1990–2016. [(accessed on 28 May 2022)]. Available online: http://www.cenaprece.salud.gob.mx/programas/interior/micobacteriosis/des....
LinkOut - more resources
Full Text Sources
