

Pembrolizumab-Induced Fatal Myasthenia, Myocarditis, and Myositis in a Patient with Metastatic Melanoma: Autopsy, Histological, and Immunohistochemical Findings-A Case Report and Literature Review
- PMID: 37446095
- PMCID: PMC10342066
- DOI: 10.3390/ijms241310919
Pembrolizumab-Induced Fatal Myasthenia, Myocarditis, and Myositis in a Patient with Metastatic Melanoma: Autopsy, Histological, and Immunohistochemical Findings-A Case Report and Literature Review
Abstract
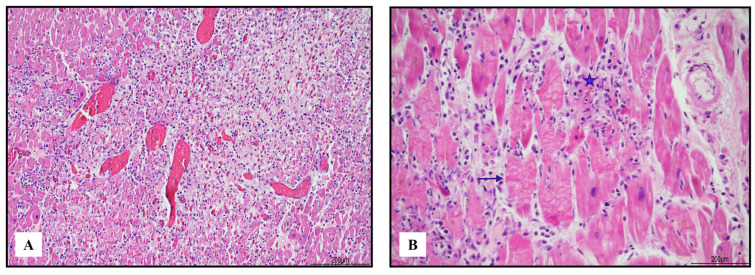
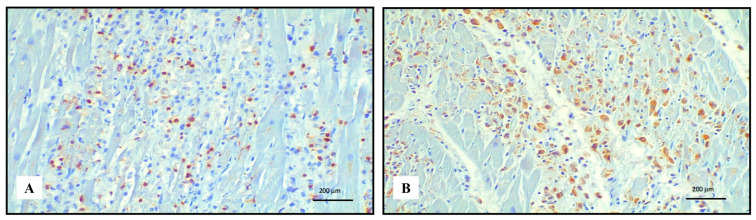
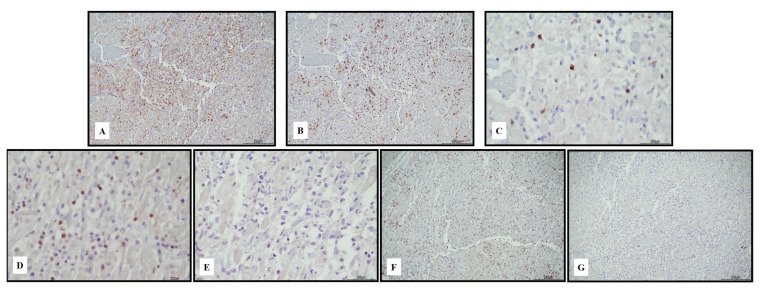
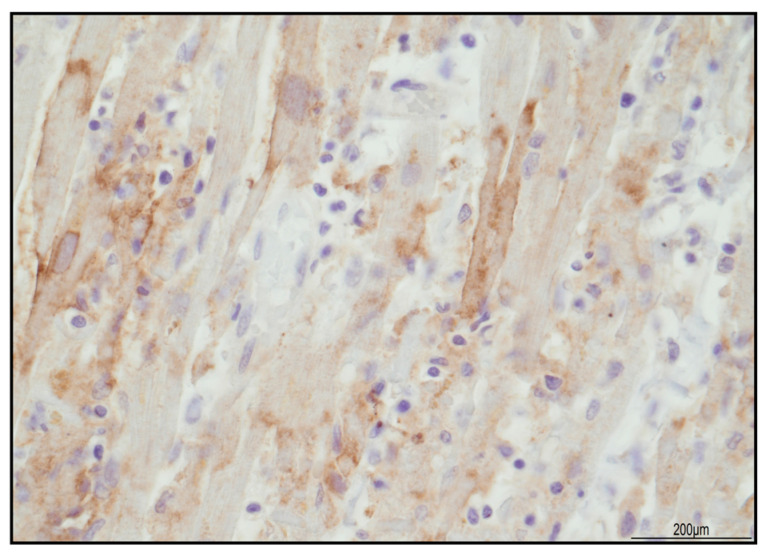
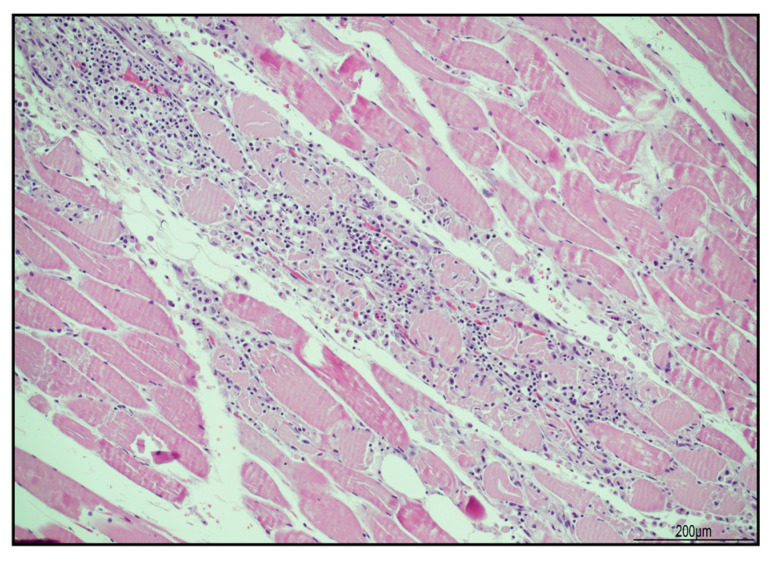
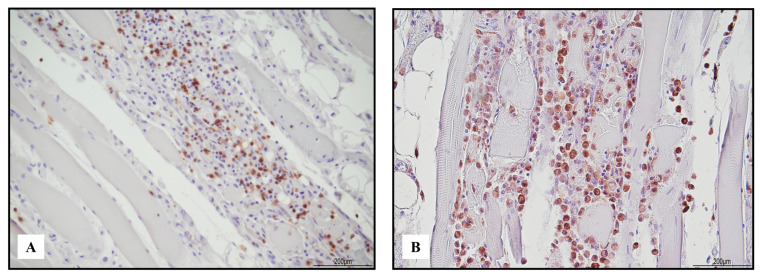
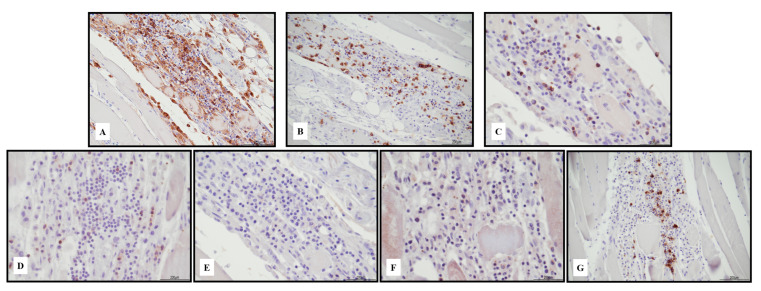
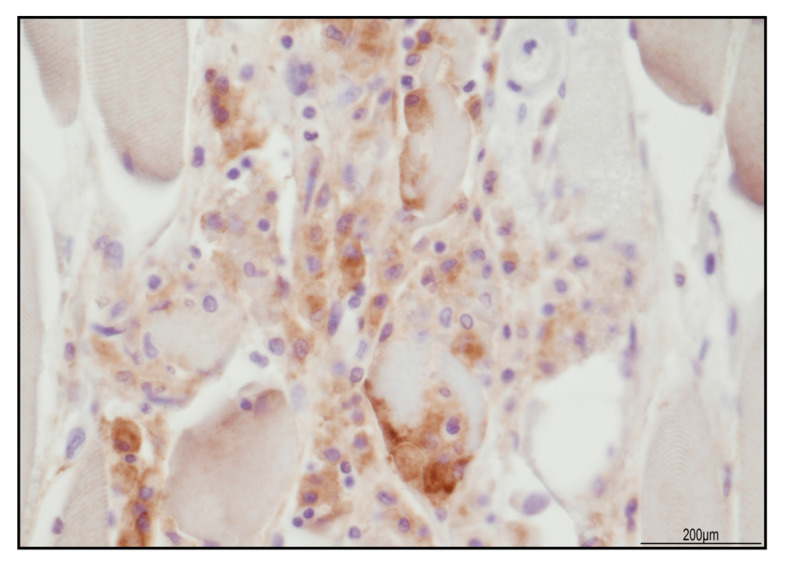
Immune checkpoint inhibitors (ICIs) represent a major advance in cancer treatment. The lowered immune tolerance induced by ICIs brought to light a series of immune-related adverse events (irAEs). Pembrolizumab belongs to the ICI class and is a humanized IgG4 anti-PD-1 antibody that blocks the interaction between PD-1 and PD-L1. The ICI-related irAEs involving various organ systems and myocarditis are uncommon (incidence of 0.04% to 1.14%), but they are associated with a high reported mortality. Unlike idiopathic inflammatory myositis, ICI-related myositis has been reported to frequently co-occur with myocarditis. The triad of myasthenia, myositis, and myocarditis must not be underestimated as they can rapidly deteriorate, leading to death. Herein we report a case of a patient with metastatic melanoma who fatally developed myasthenia gravis, myocarditis, and myositis, after a single cycle of pembrolizumab. Considering evidence from the literature review, autopsy, histological, and immunohistochemical investigations on heart and skeletal muscle are presented and discussed, also from a medical-legal perspective.
Keywords: autopsy; immunohistochemistry; myasthenia; myocarditis; myositis; pembrolizumab.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
A Fatal Case of Myocarditis Following Myositis Induced by Pembrolizumab Treatment for Metastatic Upper Urinary Tract Urothelial Carcinoma.Int Heart J. 2020 Sep 29;61(5):1070-1074. doi: 10.1536/ihj.20-162. Epub 2020 Sep 12. Int Heart J. 2020. PMID: 32921673
-
Myositis as a neuromuscular complication of immune checkpoint inhibitors.Acta Neurol Belg. 2020 Apr;120(2):355-364. doi: 10.1007/s13760-020-01282-w. Epub 2020 Jan 29. Acta Neurol Belg. 2020. PMID: 31993961
-
Nivolumab-associated myositis myocarditis and myasthenia and anti-striated muscle antibodies.Intern Med J. 2020 Aug;50(8):1003-1006. doi: 10.1111/imj.14946. Intern Med J. 2020. PMID: 33306231
-
Immune Checkpoint Inhibitor-Induced Myositis: a Case Report and Literature Review.Curr Rheumatol Rep. 2019 Feb 21;21(4):10. doi: 10.1007/s11926-019-0811-3. Curr Rheumatol Rep. 2019. PMID: 30790071 Review.
-
Pembrolizumab-induced myocarditis with complete atrioventricular block and concomitant myositis in a metastatic bladder cancer patient: a case report and review of the literature.J Med Case Rep. 2024 Feb 22;18(1):107. doi: 10.1186/s13256-024-04397-3. J Med Case Rep. 2024. PMID: 38383436 Free PMC article. Review.
Cited by
-
Pembrolizumab-associated myositis with striking extraocular muscle contrast enhancement.Acta Neurol Belg. 2024 Oct;124(5):1687-1689. doi: 10.1007/s13760-024-02589-8. Epub 2024 Jun 28. Acta Neurol Belg. 2024. PMID: 38943007 No abstract available.
-
The role of immune checkpoints PD-1 and CTLA-4 in cardiovascular complications leading to heart failure.Front Immunol. 2025 Apr 4;16:1561968. doi: 10.3389/fimmu.2025.1561968. eCollection 2025. Front Immunol. 2025. PMID: 40255399 Free PMC article. Review.
-
Management of immune-related myocarditis, myositis and myasthenia gravis (MMM) overlap syndrome: a single institution case series and literature review.Front Immunol. 2025 May 8;16:1597259. doi: 10.3389/fimmu.2025.1597259. eCollection 2025. Front Immunol. 2025. PMID: 40406130 Free PMC article. Review.
-
Myocarditis, Myositis, and Myasthenia Gravis Overlap Syndrome Associated with Immune Checkpoint Inhibitors: A Systematic Review.Diagnostics (Basel). 2024 Aug 16;14(16):1794. doi: 10.3390/diagnostics14161794. Diagnostics (Basel). 2024. PMID: 39202282 Free PMC article. Review.
References
-
- Cozma A., Sporis N.D., Lazar A.L., Buruiana A., Ganea A.M., Malinescu T.V., Berechet B.M., Fodor A., Sitar-Taut A.V., Vlad V.C., et al. Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review. Int. J. Mol. Sci. 2022;23:10948. doi: 10.3390/ijms231810948. - DOI - PMC - PubMed
-
- Nakagomi Y., Tajiri K., Shimada S., Li S., Inoue K., Murakata Y., Murata M., Sakai S., Sato K., Ieda M. Immune Checkpoint Inhibitor-Related Myositis Overlapping With Myocarditis: An Institutional Case Series and a Systematic Review of Literature. Front. Pharmacol. 2022;13:884776. doi: 10.3389/fphar.2022.884776. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
