

Survival Extrapolation Incorporating General Population Mortality Using Excess Hazard and Cure Models: A Tutorial
- PMID: 37448102
- PMCID: PMC10422853
- DOI: 10.1177/0272989X231184247
Survival Extrapolation Incorporating General Population Mortality Using Excess Hazard and Cure Models: A Tutorial
Abstract
Background: Different parametric survival models can lead to widely discordant extrapolations and decision uncertainty in cost-effectiveness analyses. The use of excess hazard (EH) methods, which incorporate general population mortality data, has the potential to reduce model uncertainty. This review highlights key practical considerations of EH methods for estimating long-term survival.
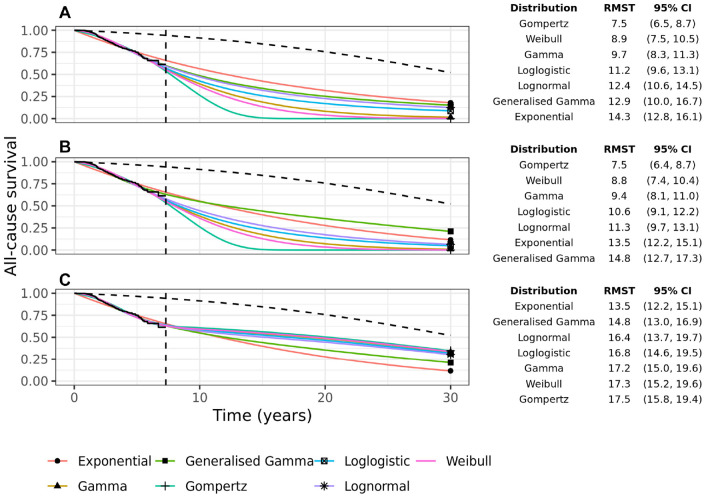
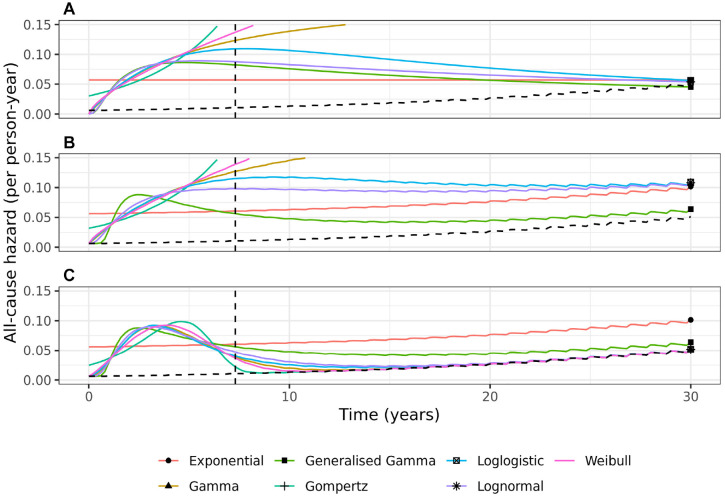
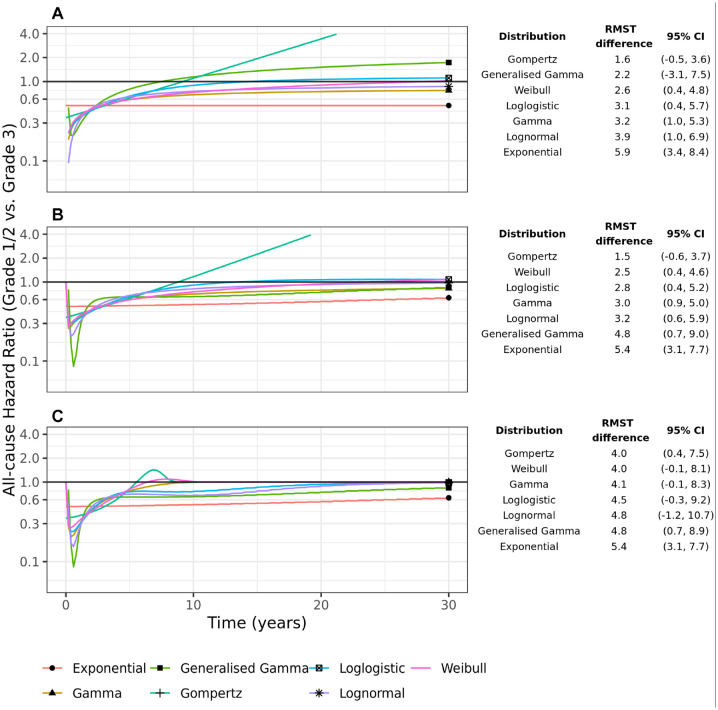
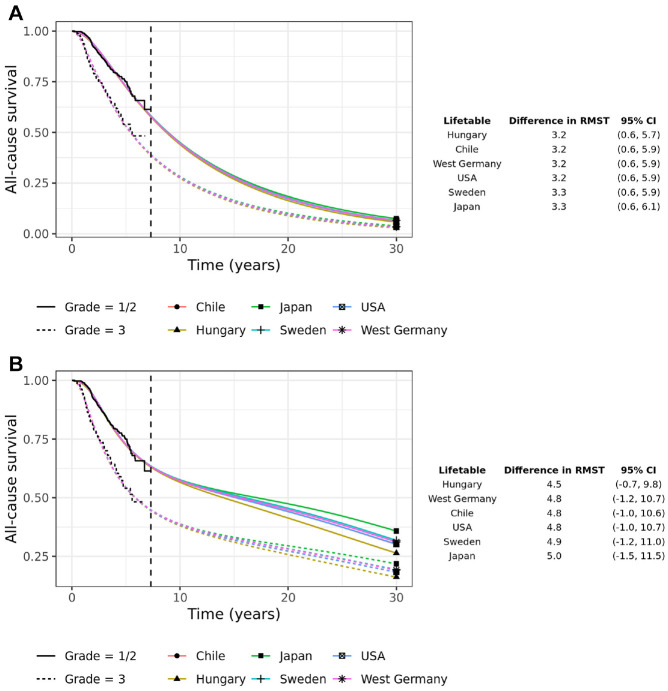
Methods: Demonstration of methods used a case study of 686 patients from the German Breast Cancer Study Group, followed for a maximum of 7.3 y and divided into low (1/2) and high (3) grade cancers. Seven standard parametric survival models were fit to each group separately. The same 7 distributions were then used in an EH framework, which incorporated general population mortality rates, and fitted both with and without a cure parameter. Survival extrapolations, restricted mean survival time (RMST), and difference in RMST between high and low grades were compared up to 30 years along with Akaike information criterion goodness-of-fit and cure fraction estimates. The sensitivity of the EH models to lifetable misspecification was investigated.
Results: In our case study, variability in survival extrapolations was extensive across the standard models, with 30-y RMST ranging from 7.5 to 14.3 y. Incorporation of general population mortality rates using EH cure methods substantially reduced model uncertainty, whereas EH models without cure had less of an effect. Long-term treatment effects approached the null for most models but at varying rates. Lifetable misspecification had minimal effect on RMST differences.
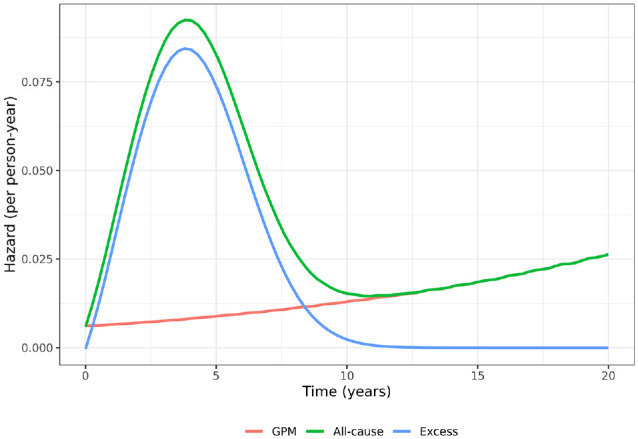
Conclusions: EH methods may be useful for survival extrapolation, and in cancer, EHs may decrease over time and be easier to extrapolate than all-cause hazards. EH cure models may be helpful when cure is plausible and likely to result in less extrapolation variability.
Highlights: In health economic modeling, to help anchor long-term survival extrapolation, it has been recommended that survival models incorporate background mortality rates using excess hazard (EH) methods.We present a thorough description of EH methods with and without the assumption of cure and demonstrate user-friendly software to aid researchers wishing to use these methods.EH models are applied to a case study, and we demonstrate that EHs are easier to extrapolate and that the use of the EH cure model, when cure is plausible, can reduce extrapolation variability.EH methods are relatively robust to lifetable misspecification.
Keywords: excess hazard models; health technology assessment; modeling; overall survival; survival extrapolation.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MJS, DJ, and RH report full-time employment with AstraZeneca and AstraZeneca stock ownership. MJR reports grants from Cancer Research UK during the conduct of the study. NRL reports grants from Yorkshire Cancer Research, grants from Bristol-Myers Squibb, grants from Merck, Sharpe and Dohme, outside the submitted work. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by a contract with AstraZeneca. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The following authors are employed by the sponsor: MJS, DJ, RH. This work was supported by Cancer Research UK grants for MJR (grant C41379/A27583). This study was further supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration East Midlands (ARC EM) and Leicester NIHR Biomedical Research Centre (BRC). The views expressed are those of the authors and not necessarily those of the NIHR and the Department of Health and Social Care.
Figures
References
-
- National Institute for Health and Care Excellence. Guide to the methods of technology appraisal 2013. Process and methods [PMG9]. April 2013. Available from: https://www.nice.org.uk/process/pmg9/chapter/foreword - PubMed
-
- Latimer N. NICE DSU Technical Support Document 14: Undertaking Survival Analysis for Economic Evaluation Alongside Clinical Trials - Extrapolation with Patient-Level Data. Report. London: National Institute for Health and Care Excellence; 2011. - PubMed
-
- Kearns B, Stevens J, Ren S, Brennan A. How uncertain is the survival extrapolation? A study of the impact of different parametric survival models on extrapolated uncertainty about hazard functions, lifetime mean survival and cost effectiveness. Pharmacoeconomics. 2020;38(2):193–204. DOI: 10.1007/s40273-019-00853-x - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
