

Anterior selective scalenectomy for periforaminal exposure in the ventral supraclavicular approach
- PMID: 37448504
- PMCID: PMC10336902
- DOI: 10.4103/jcvjs.jcvjs_153_22
Anterior selective scalenectomy for periforaminal exposure in the ventral supraclavicular approach
Abstract
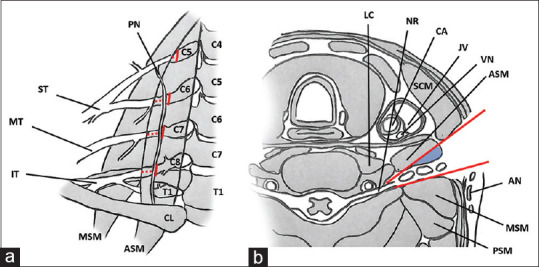
Aims and objectives: Route of choice to access cervical paravertebral lesions with foraminal involvement is the anterolateral corridor with its variants. Main limitation of these techniques is represented by the limited surgical access to periforaminal area due to the bulk generated by the anterior scalene muscle (ASM). Over the years, alternative techniques for ASM surgical management have been developed, which are still today a matter of debate. Most popular include ASM scalene complete section (SCS) and ASM medial detachment (SMD). Authors describe an innovative, minimally invasive muscle section technique, the anterior selective scalenectomy (ASS), which reduces the risk of iatrogenic morbidity and optimizes exposure of periforaminal area in anterolateral cervical routes.
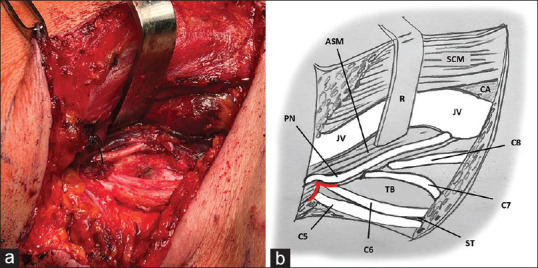
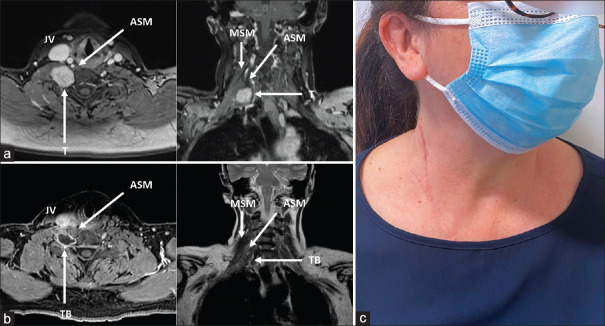
Materials and methods: A laboratory investigation was conducted. Technique was applied in a surgical setting, and an illustrative case was reported.
Results: ASS is a quick and easy technique to perform. It allows optimization of surgical visibility and control on the periforaminal area in the cervical anterolateral corridor. It respects muscle anatomy and vascularization, favoring functional recovery and management of peri-operative pain; it reduces the risk of morbidity on phrenic nerve and pleura. Considering the minimally invasive nature of the technique, it allows for a slightly more limited exposure compared to traditional techniques while ensuring optimal surgical maneuverability on the target area.
Conclusions: ASS represents an effective and safe alternative to traditional ASM section techniques for the exposure of periforaminal area in anterolateral cervical routes. It is indicated in case of lesions with paravertebral development and minimal intraforaminal component in the C3-C6 segment.
Keywords: Brachial plexus; cervical anterolateral approach; cervical paravertebral tumors; scalenectomy; ventral supraclavicular approach.
Copyright: © 2023 Journal of Craniovertebral Junction and Spine.
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
References
-
- Binder DK, Smith JS, Barbaro NM. Primary brachial plexus tumors: Imaging, surgical, and pathological findings in 25 patients. Neurosurg Focus. 2004;16:E11. - PubMed
-
- Das S, Ganju A, Tiel RL, Kline DG. Tumors of the brachial plexus. Neurosurg Focus. 2007;22:E26. - PubMed
-
- Huang JH, Zaghloul K, Zager EL. Surgical management of brachial plexus region tumors. Surg Neurol. 2004;61:372–8. - PubMed
-
- Jia X, Yang J, Chen L, Yu C, Kondo T. Primary brachial plexus tumors: Clinical experiences of 143 cases. Clin Neurol Neurosurg. 2016;148:91–5. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous