

Optimal anatomical angle and distance for drilling in cervical oblique corpectomy: A surgical anatomical study
- PMID: 37448508
- PMCID: PMC10336893
- DOI: 10.4103/jcvjs.jcvjs_26_23
Optimal anatomical angle and distance for drilling in cervical oblique corpectomy: A surgical anatomical study
Abstract
Background: One of the difficulties of oblique corpectomy, less discussed in the literature, is the problem of how to achieve an optimum corpectomy. Therefore, this anatomico-radiological study was conducted to shed light on the use of the microscope at an appropriate angle and optimum drill distances in clinical cases undergoing cervical oblique corpectomy surgery.
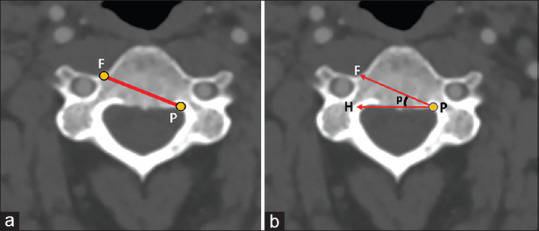
Materials and methods: We examined the average distance of the diagonal line extending from the medial aspect of the ipsilateral vertebral foramen to the contralateral pedicle in cervical computed tomography -angiography axial scans in four cervical vertebrae, C3, C4, C5, and C6. We also measured the average angle between this diagonal trajectory and the horizontal line, making a total of 712 measurements in 89 patients.
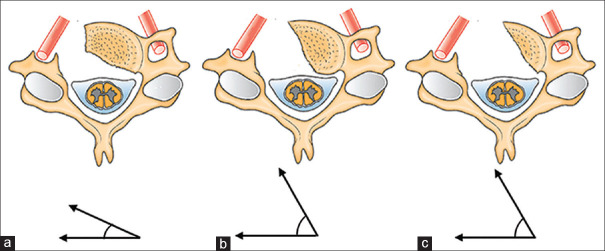
Results: We found that horizontal drilling with an average length of 23-26 mm at an acute angle of about 22° -23° is optimal for adequate decompression of the spinal cord in the oblique corpectomy approach. Depending on the patient and the level of the vertebra, the distance and the angle of the horizontal drilling may range from 18 mm to 31 mm and from 15° to 33°, respectively.
Conclusions: For an optimum cervical oblique corpectomy that provides adequate spinal cord decompression and maintains spinal stability, it is necessary to operate under a surgical microscope positioned at an acute angle and to know the horizontal drilling distance.
Keywords: Anatomy; cervical oblique corpectomy; cervical vertebrae; multilevel corpectomy; neck anatomy; surgical anatomy; vertebral anatomy.
Copyright: © 2023 Journal of Craniovertebral Junction and Spine.
Conflict of interest statement
There are no conflicts of interest.
Figures




Similar articles
-
Results of surgical treatment for degenerative cervical myelopathy: anterior cervical corpectomy and stabilization.Spine (Phila Pa 1976). 2004 Nov 15;29(22):2493-500. doi: 10.1097/01.brs.0000145412.93407.c3. Spine (Phila Pa 1976). 2004. PMID: 15543060
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Hybrid Decompression and Fixation Technique Versus Plated 3-Vertebra Corpectomy for 4-Segment Cervical Myelopathy: Analysis of 81 Cases With a Minimum 2-Year Follow-Up.Clin Spine Surg. 2016 Jul;29(6):226-33. doi: 10.1097/BSD.0b013e31827ada34. Clin Spine Surg. 2016. PMID: 23168392
-
[Anterior slip phenomenon of the vertebrae after corpectomy surgery and its clinical significance].Zhongguo Gu Shang. 2016 Oct 25;29(10):947-953. doi: 10.3969/j.issn.1003-0034.2016.10.014. Zhongguo Gu Shang. 2016. PMID: 29285915 Chinese.
-
Multilevel oblique corpectomies: surgical indications and technique.Neurosurgery. 2007 Sep;61(3 Suppl):106-12; discussion 112. doi: 10.1227/01.neu.0000289723.89588.72. Neurosurgery. 2007. PMID: 17876240 Review.
References
-
- Durrani S, Onyedimma C, Jarrah R, Bhatti A, Nathani KR, Bhandarkar AR, et al. The virtual vision of neurosurgery: How augmented reality and virtual reality are transforming the neurosurgical operating room. World Neurosurg. 2022;168:190–201. - PubMed
-
- Balak N, Baran O, Denli Yalvac ES, Esen Aydin A, Kumbasar A, Tanriover N. Cervical oblique corpectomy: Revitalizing the underused surgical approach with step-by-step simulation in cadavers. J Craniofac Surg. 2022;33:337–43. - PubMed
-
- Henry AK. Exposures of Long Bones and Other Surgical Methods. London: J Wright and Sons, Limited; Simpkin, Marshall, Hamilton, Kent and Company, Limited; 1927.
LinkOut - more resources
Full Text Sources
Miscellaneous