

Oncoplastic and reconstructive breast surgery
- PMID: 37448512
- PMCID: PMC10338173
- DOI: 10.3389/fonc.2023.1176915
Oncoplastic and reconstructive breast surgery
Abstract
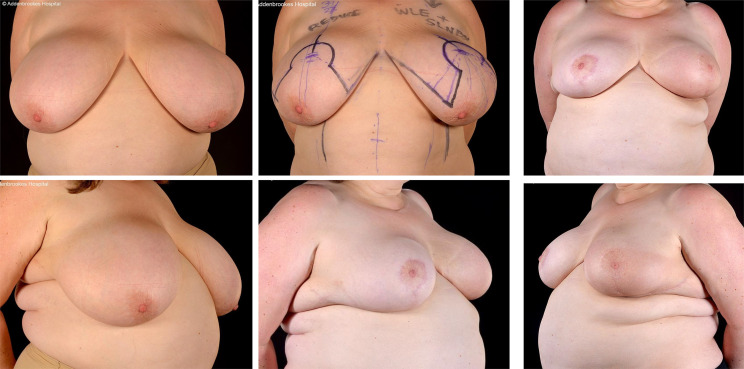
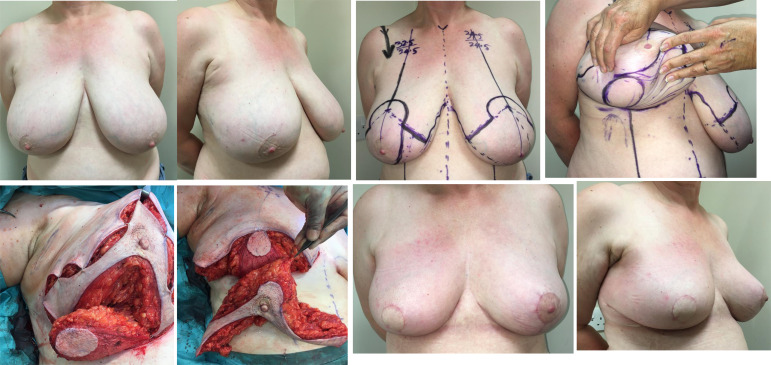
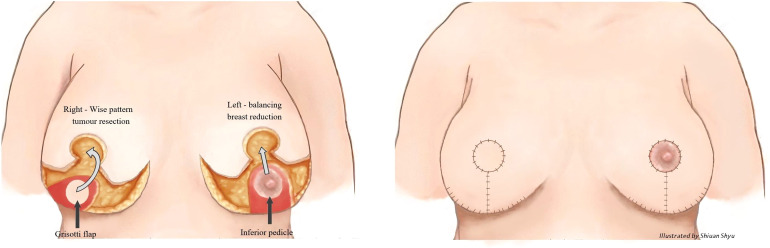
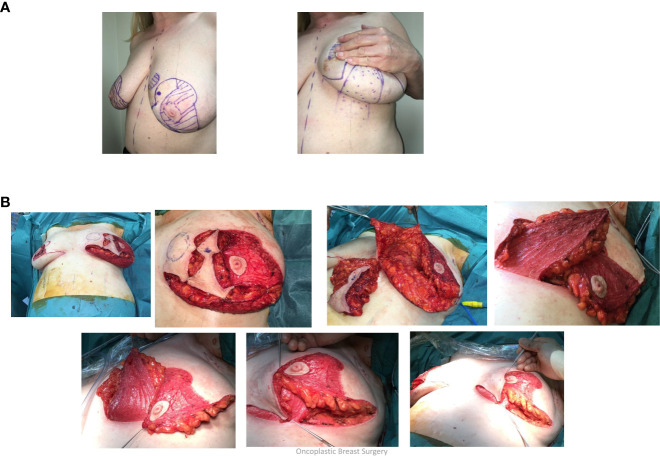
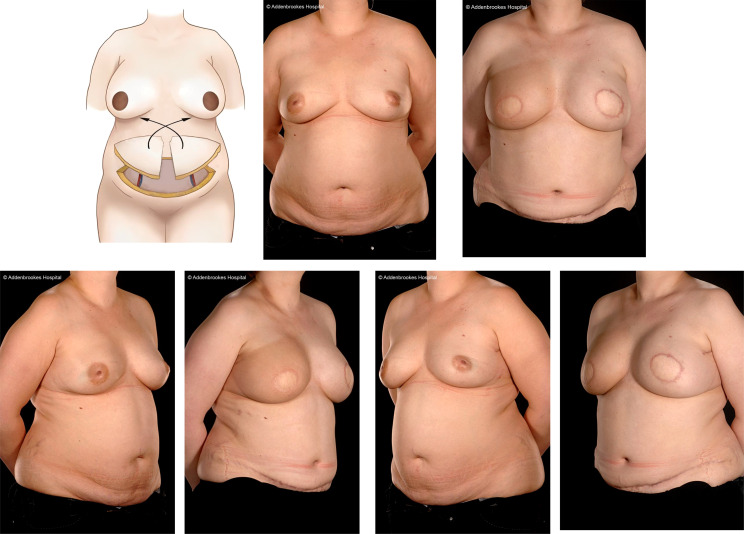
This article provides an overview of the principles and techniques of oncoplastic and reconstructive breast surgery for patients with early-stage breast cancer. Oncoplastic breast surgery (OPBS) with partial breast reconstruction is a natural evolution in the application of breast conserving surgery and permits wide surgical resection of tumours that might otherwise mandate mastectomy and whole breast reconstruction. These reconstructive techniques must be optimally selected and integrated with ablative breast surgery together with non-surgical treatments such as radiotherapy and chemotherapy that may be variably sequenced with each other. A multidisciplinary approach with shared decision-making is essential to ensure optimal clinical and patient-reported outcomes that address oncological, aesthetic, functional and psychosocial domains. Future practice of OPBS must incorporate routine audit and comprehensive evaluation of outcomes.
Keywords: autologous free flap; breast implants; breast reconstruction; fat grafting; nipple sparing mastectomy; oncoplastic breast surgery.
Copyright © 2023 Wignarajah, Malata and Benson.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Facts and figures | breast cancer UK. Available at: https://www.breastcanceruk.org.uk/about-breast-cancer/facts-figures-and-....
-
- Breast cancer. Available at: https://www.who.int/news-room/fact-sheets/detail/breast-cancer.
-
- Breast cancer statistics and facts | breast cancer now. Available at: https://breastcancernow.org/about-us/media/facts-statistics.
Publication types
LinkOut - more resources
Full Text Sources