

Acute shortening and angulation for complex open fractures: an updated perspective
- PMID: 37448568
- PMCID: PMC10337845
- DOI: 10.1097/OI9.0000000000000245
Acute shortening and angulation for complex open fractures: an updated perspective
Abstract
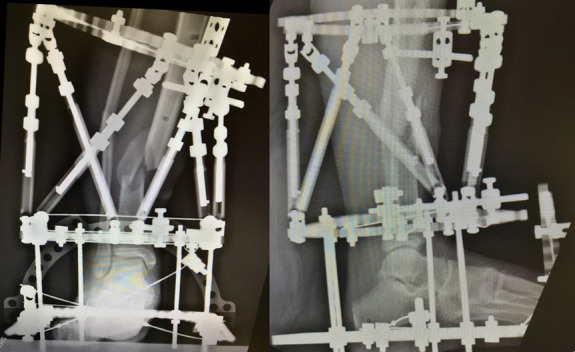
Reestablishing an intact, healthy soft tissue envelope is a critical step in managing lower extremity injuries, particularly high-grade open tibia fractures. Acute shortening and angulation can be used independently or together to address complex soft tissue injuries, particularly when bone loss is present. These techniques facilitate management of difficult wounds and can be combined with local soft tissue rearrangement or pedicled flaps as needed, avoiding the need for free tissue transfer. After angular deformity correction, adjacent bone loss can be addressed with bone grafting or distraction histogenesis. This article discusses the indications for, surgical technique for, and limitations of acute shortening and angulation for management of open lower extremity fractures.
Keywords: angulation; distraction histogenesis; distraction osteogenesis; hexapod frame; induced deformity; open fracture; shortening; tibia fracture.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Orthopaedic Trauma Association.
Conflict of interest statement
This manuscript is original, has not been published previously, and is not being considered for publication elsewhere. Neither author has conflicts of interest, financial or otherwise, associated with this publication.
Figures


References
-
- Lerner A, Fodor L, Soudry M, et al. Acute shortening: modular treatment modality for severe combined bone and soft tissue loss of the extremities. J Trauma 2004;57:603–608. - PubMed
-
- Beltran MJ, Blair JA, Rathbone CR, et al. The gradual expansion muscle flap. J Orthop Trauma. 2014;28:e15–e20. - PubMed
-
- Hsu JR, Beltran MJ, STReC. Shortening and angulation for soft-tissue reconstruction of extremity wounds at a combat support hospital. Mil Med 2009;174:838–842. - PubMed
-
- Thakeb MF, Fayyad TA, ElGebeily MA, et al. Bifocal compression-distraction for combined bone and soft-tissue defects in post-traumatic tibial nonunion. J Orthop Trauma. 2019;33:e372–e377. - PubMed
-
- Beltran MJ, Ochoa LM, Graves RM, et al. Composite bone and soft tissue loss treated with distraction histiogenesis. J Surg Orthop Adv. 2010;19:23–28. - PubMed
Publication types
LinkOut - more resources
Full Text Sources