

Home-based exercise training by using a smartphone app in patients with Parkinson's disease: a feasibility study
- PMID: 37448748
- PMCID: PMC10338039
- DOI: 10.3389/fneur.2023.1205386
Home-based exercise training by using a smartphone app in patients with Parkinson's disease: a feasibility study
Abstract
Background: Parkinson's disease (PD) patients experience deterioration in mobility with consequent inactivity and worsened health and social status. Physical activity and physiotherapy can improve motor impairments, but several barriers dishearten PD patients to exercise regularly. Home-based approaches (e.g., via mobile apps) and remote monitoring, could help in facing this issue.
Objective: This study aimed at testing the feasibility, usability and training effects of a home-based exercise program using a customized version of Parkinson Rehab® application.
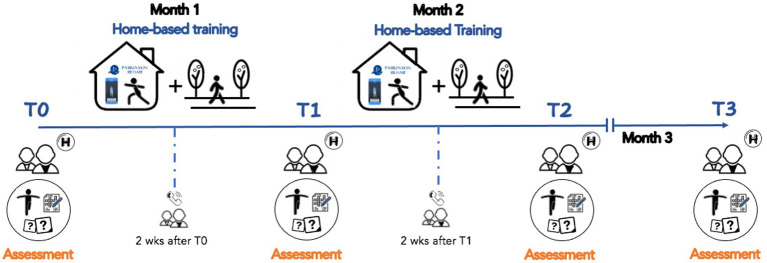
Methods: Twenty PD subjects participated in a two-month minimally supervised home-based training. Daily session consisted in performing PD-specific exercises plus a walking training. We measured: (i) feasibility (training adherence), usability and satisfaction (via an online survey); (ii) safety; (iii) training effects on PD severity, mobility, cognition, and mood. Evaluations were performed at: baseline, after 1-month of training, at the end of training (T2), and at 1-month follow-up (T3).
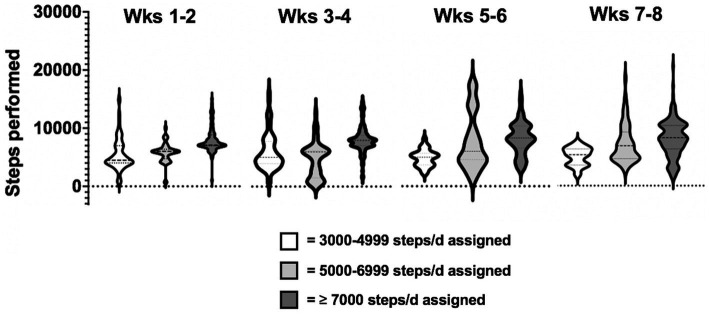
Results: Eighteen out of twenty participants completed the study without important adverse events. Participants' adherence was 91% ± 11.8 for exercise and 105.9% ± 30.6 for walking training. Usability and satisfaction survey scored 70.9 ± 7.7 out of 80. Improvements in PD severity, mobility and cognition were found at T2 and maintained at follow-up.
Conclusion: The home-based training was feasible, safe and seems to positively act on PD-related symptoms, mobility, and cognition in patients with mild to moderate stage of PD disease. Additionally, the results suggest that the use of a mobile app might increase the amount of daily physical activity in our study population. Remote monitoring and tailored exercise programs appear to be key elements for promoting exercise. Future studies in a large cohort of PD participants at different stages of disease are needed to confirm these findings.
Keywords: Parkinson disease; exercise; gait; home-based training; mobile apps.
Copyright © 2023 Putzolu, Manzini, Gambaro, Cosentino, Bonassi, Botta, Ravizzotti, Avanzino, Pelosin and Mezzarobba.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- GBD 2016 Neurology collaborators. Feigin VL, Nichols E, Alam T, Bannick MS, Beghi E, et al. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:459–11. doi: 10.1016/S1474-4422(18)30499-X, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources