

Comparison of 3D and 4D robustly optimized proton treatment plans for non-small cell lung cancer patients with tumour motion amplitudes larger than 5 mm
- PMID: 37449022
- PMCID: PMC10338142
- DOI: 10.1016/j.phro.2023.100465
Comparison of 3D and 4D robustly optimized proton treatment plans for non-small cell lung cancer patients with tumour motion amplitudes larger than 5 mm
Abstract
Background and purpose: There is no consensus about an ideal robust optimization (RO) strategy for proton therapy of targets with large intrafractional motion. We investigated the plan robustness of 3D and different 4D RO strategies.
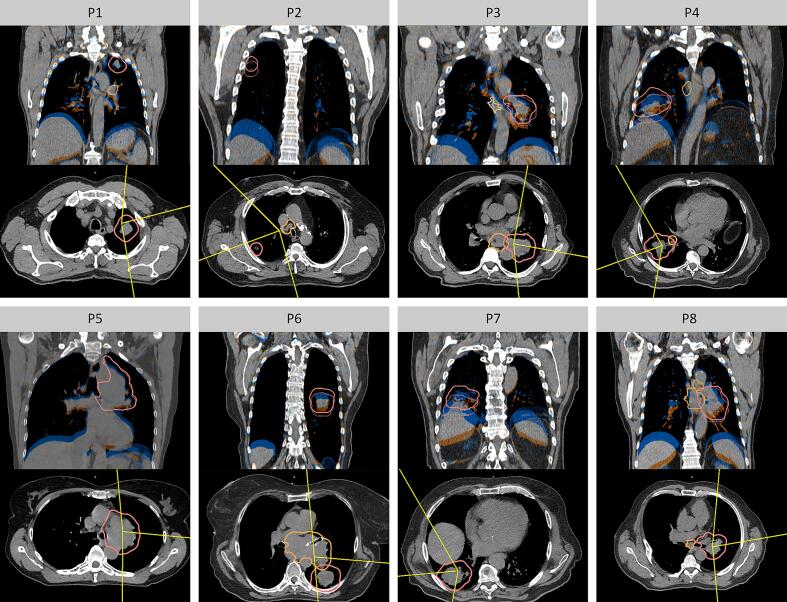
Materials and methods: For eight non-small cell lung cancer patients with clinical target volume (CTV) motion >5 mm, different RO approaches were investigated: 3DRO considering the average CT (AvgCT) with a target density override, 4DRO considering three/all 4DCT phases, and 4DRO considering the AvgCT and three/all 4DCT phases. Robustness against setup/range errors, interplay effects based on breathing and machine log file data for deliveries with/without rescanning, and interfractional anatomical changes were analyzed for target coverage and OAR sparing.
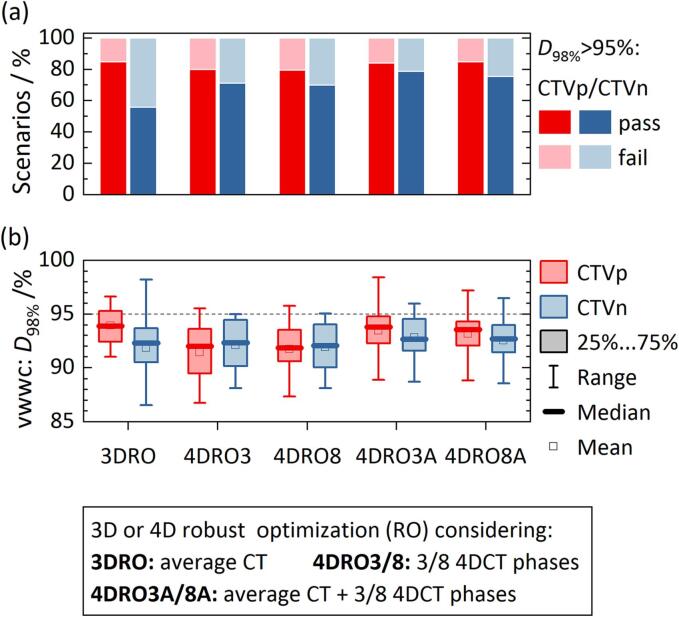
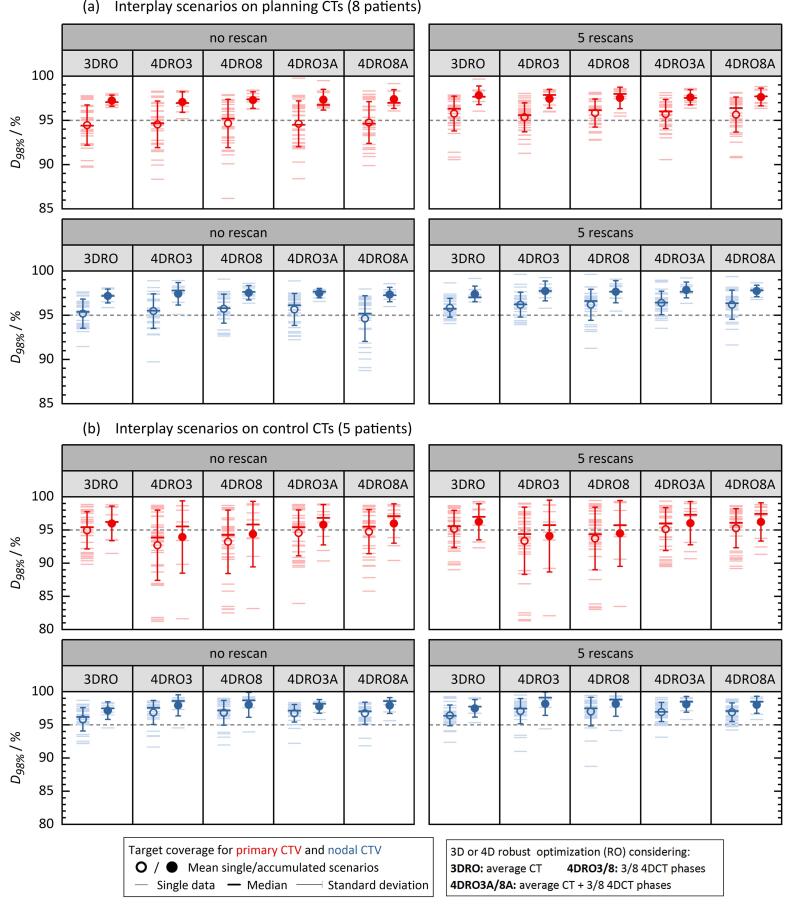
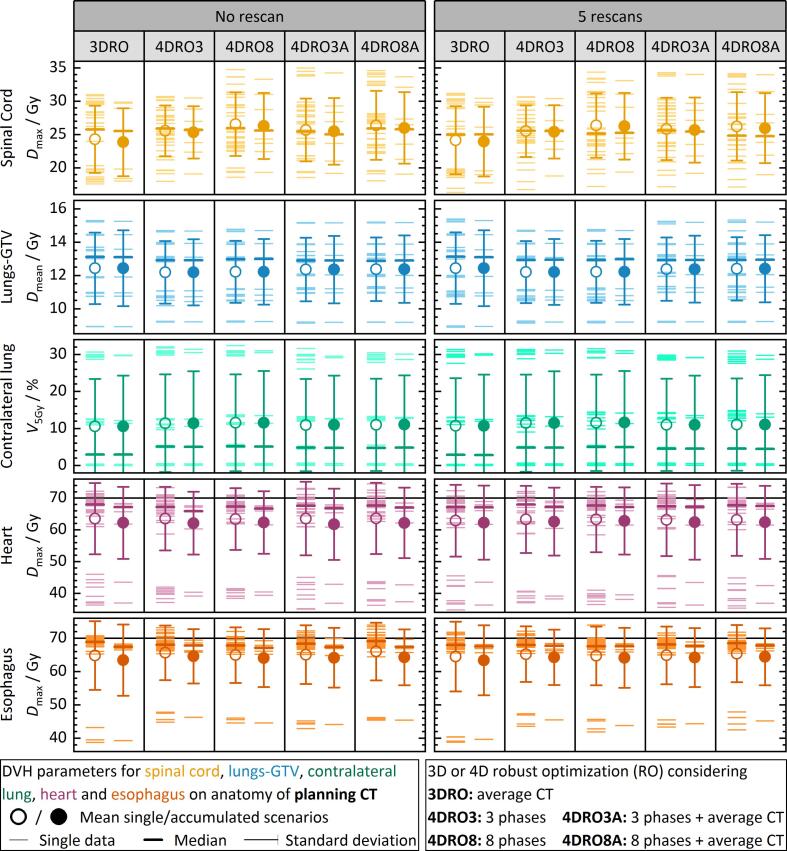
Results: All nominal plans fulfilled the clinical requirements with individual CTV coverage differences <2pp; 4DRO without AvgCT generated the most conformal dose distributions. Robustness against setup/range errors was best for 4DRO with AvgCT (18% more passed error scenarios than 3DRO). Interplay effects caused fraction-wise median CTV coverage loss of 3pp and missed maximum dose constraints for heart and esophagus in 18% of scenarios. CTV coverage and OAR sparing fulfilled requirements in all cases when accumulating four interplay scenarios. Interfractional changes caused less target misses for RO with AvgCT compared to 4DRO without AvgCT (≤42%/33% vs. ≥56%/44% failed single/accumulated scenarios).
Conclusions: All RO strategies provided acceptable plans with equally low robustness against interplay effects demanding other mitigation than rescanning to ensure fraction-wise target coverage. 4DRO considering three phases and the AvgCT provided best compromise on planning effort and robustness.
Keywords: Interfraction changes; Large intrafraction motion; Lung cancer; Proton therapy; Robust optimization.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Lu H-M, Brett R, Sharp G, Safai S, Jiang S, Madden T, et al. The development and commissioning of a respiratory-gated treatment system for proton therapy. In: Magjarevic R, Nagel JH, editors. World Congr. Med. Phys. Biomed. Eng. 2006, vol. 14. Berlin, Heidelberg: Springer Berlin Heidelberg; 2007. p. 2215–8. 10.1007/978-3-540-36841-0_559. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
