

Role of ST-Segment Resolution Alone and in Combination With TIMI Flow After Primary Percutaneous Coronary Intervention for ST-Segment-Elevation Myocardial Infarction
- PMID: 37449560
- PMCID: PMC10382099
- DOI: 10.1161/JAHA.123.029670
Role of ST-Segment Resolution Alone and in Combination With TIMI Flow After Primary Percutaneous Coronary Intervention for ST-Segment-Elevation Myocardial Infarction
Abstract
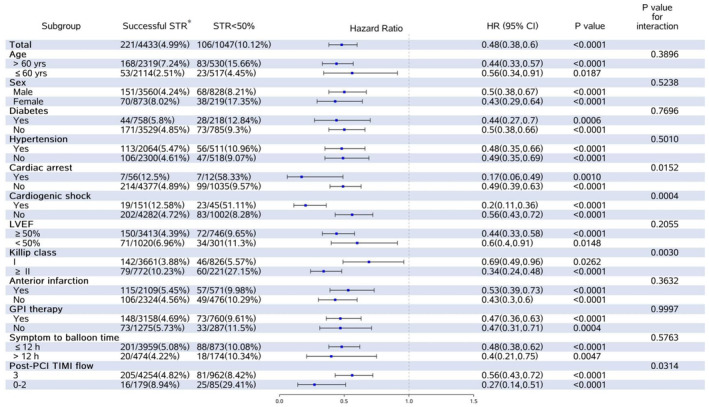
Background To evaluate the role of ST-segment resolution (STR) alone and in combination with Thrombolysis in Myocardial Infarction (TIMI) flow in reperfusion evaluation after primary percutaneous coronary intervention (PPCI) for ST-segment-elevation myocardial infarction by investigating the long-term prognostic impact. Methods and Results From January 2013 through September 2014, we studied 5966 patients with ST-segment-elevation myocardial infarction enrolled in the CAMI (China Acute Myocardial Infarction) registry with available data of STR evaluated at 120 minutes after PPCI. Successful STR included STR ≥50% and complete STR (ST-segment back to the equipotential line). After PPCI, the TIMI flow was assessed. The primary outcome was 2-year all-cause mortality. STR < 50%, STR ≥50%, and complete STR occurred in 20.6%, 64.3%, and 15.1% of patients, respectively. By multivariable analysis, STR ≥50% (5.6%; adjusted hazard ratio [HR], 0.45 [95% CI, 0.36-0.56]) and complete STR (5.1%; adjusted HR, 0.48 [95% CI, 0.34-0.67]) were significantly associated with lower 2-year mortality than STR <50% (11.7%). Successful STR was an independent predictor of 2-year mortality across the spectrum of clinical variables. After combining TIMI flow with STR, different 2-year mortality was observed in subgroups, with the lowest in successful STR and TIMI 3 flow, intermediate when either of these measures was reduced, and highest when both were abnormal. Conclusions Post-PPCI STR is a robust long-term prognosticator for ST-segment-elevation myocardial infarction, whereas the integrated analysis of STR plus TIMI flow yields incremental prognostic information beyond either measure alone, supporting it as a convenient and reliable surrogate end point for defining successful PPCI. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT01874691.
Keywords: ECG; acute myocardial infarction; outcome; reperfusion.
Figures


References
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, et al. 2013 ACCF/AHA guideline for the management of ST‐elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–e425. doi: 10.1161/CIR.0b013e3182742cf6 - DOI - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli‐Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2017;39:119–177. doi: 10.1093/eurheartj/ehx393 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
