

Interdisciplinary perspectives on computed tomography in sepsis: survey among medical doctors at a large university medical center
- PMID: 37450054
- PMCID: PMC10667150
- DOI: 10.1007/s00330-023-09842-3
Interdisciplinary perspectives on computed tomography in sepsis: survey among medical doctors at a large university medical center
Abstract
Objectives: This study aims to describe physicians' perspectives on the use of computed tomography (CT) in patients with sepsis.
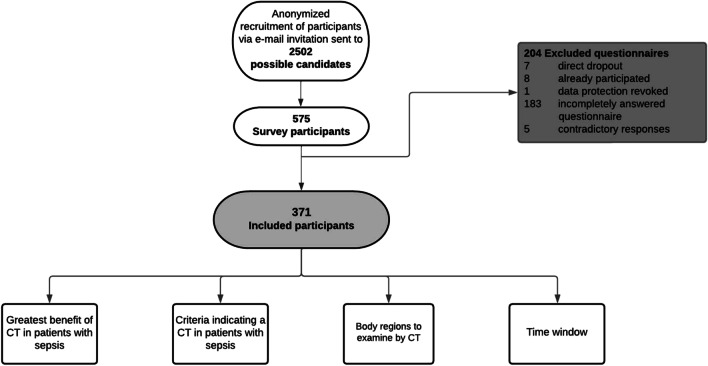
Methods: In January 2022, physicians of a large European university medical center were surveyed using a web-based questionnaire asking about their views on the role of CT in sepsis. A total of 371 questionnaires met the inclusion criteria and were analyzed using work experience, workplace, and medical specialty of physicians as variables. Chi-square tests were performed.
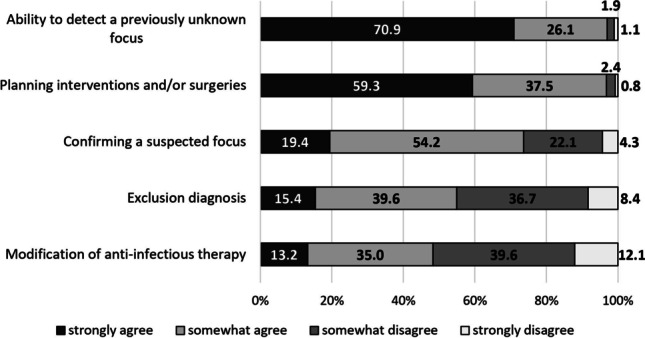
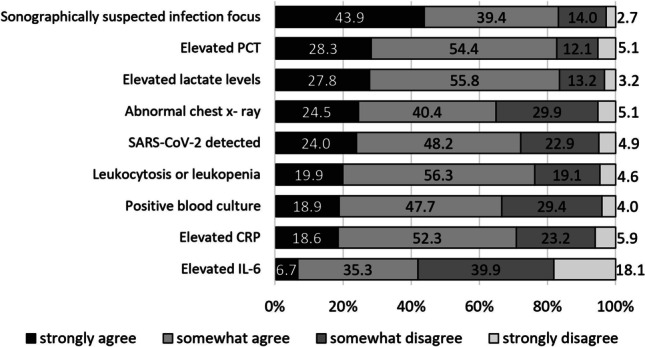
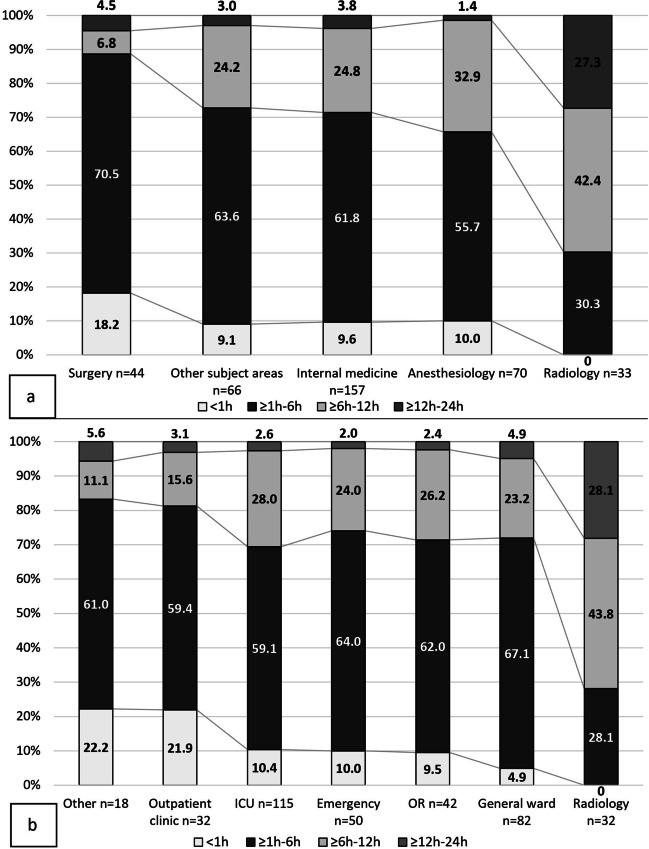
Results: Physicians considered the ability to detect an unknown focus as the greatest benefit of CT scans in sepsis (70.9%, n = 263/371). Two clinical criteria - "signs of decreased vigilance" (89.2%, n = 331/371) and "increased catecholamine demand" (84.7%, n = 314/371) - were considered highly relevant for a CT request. Elevated procalcitonin (82.7%, n = 307/371) and lactate levels (83.6%, n = 310/371) were consistently found to be critical laboratory values to request a CT. As long as there is evidence of infection in one organ region, most physicians (42.6%, n = 158/371) would order a CT scan based on clinical assessment. Combined examination of the chest, abdomen, and pelvis was favored (34.8%, n = 129/371) in cases without clinical clues of an infection source. A time window of ≥ 1-6 h was preferred for both CT examinations (53.9%, n = 200/371) and CT-guided interventions (59.3%, n = 220/371) in patients with sepsis.
Conclusion: Despite much consensus, there are significant differences in attitudes towards the use of CT in septic patients among physicians from different workplaces and medical specialties. Knowledge of these perspectives may improve patient management and interprofessional communication.
Key points: Despite interdisciplinary consensus on the use of CT in sepsis, statistically significant differences in the responses are apparent among physicians from different workplaces and medical specialties. The detection of a previously unknown source of infection and the ability to plan interventions and/or surgery based on CT findings are considered key advantages of CT in septic patients. Timing of CT reflects the requirements of specific disciplines.
Keywords: Clinical reasoning; Physicians; Sepsis; Surveys and questionnaires; Tomography, X-ray computed.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures


References
-
- Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (2018) S3-Leitlinie Sepsis – Prävention, Diagnose, Therapie und Nachsorge. Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften, Frankfurt am Main. Available via https://www.awmf.org/uploads/tx_szleitlinien/079-001l_S3_Sepsis-Praevent.... Accessed 18 Sept 2021
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
