

The Development of Ofatumumab, a Fully Human Anti-CD20 Monoclonal Antibody for Practical Use in Relapsing Multiple Sclerosis Treatment
- PMID: 37450172
- PMCID: PMC10444716
- DOI: 10.1007/s40120-023-00518-0
The Development of Ofatumumab, a Fully Human Anti-CD20 Monoclonal Antibody for Practical Use in Relapsing Multiple Sclerosis Treatment
Abstract
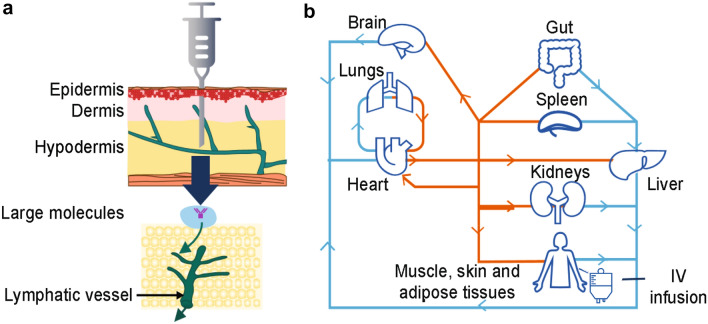
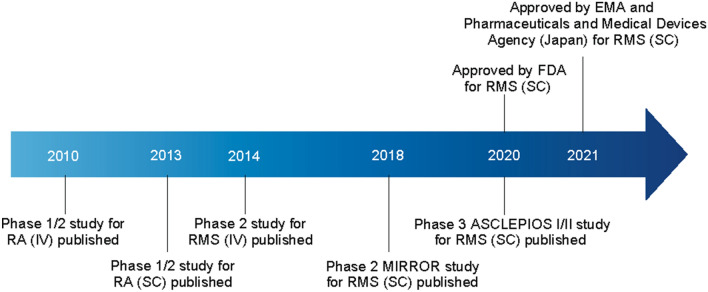
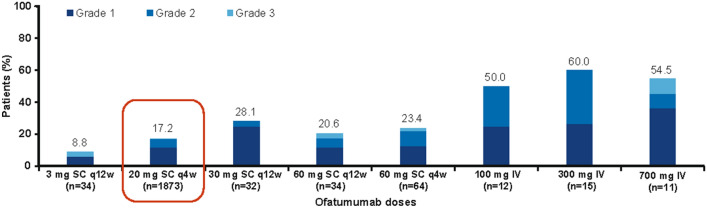
The importance of B cells in multiple sclerosis (MS) has been demonstrated through the advent of B-cell-depleting anti-CD20 antibody therapies. Ofatumumab is the first fully human anti-CD20 monoclonal antibody (mAb) developed and tested for subcutaneous (SC) self-administration at monthly doses of 20 mg, and has been approved in the US, UK, EU, and other regions and countries worldwide for the treatment of relapsing MS. The development goal of ofatumumab was to obtain a highly efficacious anti-CD20 therapy, with a safety and tolerability profile that allows for self-administration by MS patients at home and a positive benefit-risk balance for use in the broad relapsing MS population. This development goal was enabled by the unique binding site, higher affinity to B cells, and higher potency of ofatumumab compared to previous anti-CD20 mAbs; these properties of ofatumumab facilitate rapid B-cell depletion and maintenance with a low dose at a low injection volume (20 mg/0.4 ml). The high potency in turn enables the selective targeting of B cells that reside in the lymphatic system via subcutaneous (SC) administration. Through a comprehensive dose-finding program in two phase 2 studies (one intravenous and one SC) and model simulations, it was found that safety and tolerability can be further improved, and the risk of systemic injection-related reactions (IRRs) minimized, by avoiding doses ≥ 30 mg, and by reaching initial and rapid B-cell depletion via stepwise weekly administration of ofatumumab at Weeks 0, 1, and 2 (instead of a single high dose). Once near-complete B-cell depletion is reached, it can be maintained by monthly doses of 20 mg/0.4 ml. Indeed, in phase 3 trials (ASCLEPIOS I/II), rapid and sustained near-complete B-cell depletion (largely independent of body weight, race and other factors) was observed with this dosing regimen, which resulted in superior efficacy of ofatumumab versus teriflunomide on relapse rates, disability worsening, neuronal injury (serum neurofilament light chain), and imaging outcomes. Likely due to its fully human nature, ofatumumab has a low immunogenic risk profile-only 2 of 914 patients receiving ofatumumab in ASCLEPIOS I/II developed anti-drug antibodies-and this may also underlie the infrequent IRRs (20% with ofatumumab vs. 15% with the placebo injection in the teriflunomide arm) that were mostly (99.8%) mild to moderate in severity. The overall rates of infections and serious infections in patients treated with ofatumumab were similar to those in patients treated with teriflunomide (51.6% vs. 52.7% and 2.5% vs. 1.8%, respectively). The benefit-risk profile of ofatumumab was favorable compared to teriflunomide in the broad RMS population, and also in the predefined subgroups of both recently diagnosed and/or treatment-naïve patients, as well as previously disease-modifying therapy-treated patients. Interim data from the ongoing extension study (ALITHIOS) have shown that long-term treatment with ofatumumab up to 4 years is well-tolerated in RMS patients, with no new safety risks identified. In parallel to the phase 3 trials in which SC administration was carried out with a pre-filled syringe, an autoinjector pen for more convenient self-administration of the ofatumumab 20 mg dose was developed and is available for use in clinical practice.
Keywords: ALITHIOS; ASCLEPIOS I/II; Anti-CD20 monoclonal antibody; Benefit-risk; Ofatumumab; Relapsing multiple sclerosis; Self-administration; Subcutaneous.
© 2023. The Author(s).
Conflict of interest statement
Stephen L. Hauser has received personal compensation from Annexon, Alector, Accure, and Neurona; he has also received travel reimbursement from F. Hoffmann-La Roche Ltd and Novartis for CD20-related meetings and presentations. Ludwig Kappos has received no personal compensation. His institutions (University Hospital Basel/Stiftung Neuroimmunology and Neuroscience Basel) have received the following exclusively for research support: steering committee, advisory board and consultancy fees (Abbvie, Actelion, Auriga Vision AG, Bayer HealthCare, Biogen, Celgene, df-mp [Dörries Frank-Molnia & Pohlman], Eli Lilly, EMD Serono, Genentech, Genzyme, Glaxo Smith Kline, Janssen, Merck, Minoryx, Novartis, Roche, Sanofi, Santhera, Senda Biosciences, Shionogi and Wellmera AG); speaker fees (Bristol Myrers Squibb, Celgene, Janssen, Merck, Novartis, and Roche); support for educational activities (Biogen, Desitin, Novartis, Sanofi and Teva); license fees for Neurostatus products; and grants (European Union, Innosuisse, Novartis, Roche, Swiss MS Society and Swiss National Research Foundation). Amit Bar-Or has participated as a speaker in meetings sponsored by, and received consulting fees and/or grant support from, Accure, Atara Biotherapeutics, Biogen, BMS/Celgene/Receptos, GlaxoSmithKline, Gossamer, Janssen/Actelion, Medimmune, Merck/EMD Serono, Novartis, Roche/Genentech, Sanofi Genzyme. Heinz Wiendl has received honoraria for acting as a member of scientific advisory boards for Biogen, Evgen, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Roche Pharma AG, and Sanofi-Aventis, as well as speaker honoraria and travel support from Alexion, Biogen, Cognomed, F. Hoffmann-La Roche Ltd., Gemeinnützige Hertie-Stiftung, Merck Serono, Novartis, Roche Pharma AG, Genzyme, Teva, and WebMD Global. Heinz Wiendl is acting as a paid consultant for AbbVie, Actelion, Biogen, IGES, Johnson & Johnson, Novartis, Roche, Sanofi-Aventis, and the Swiss Multiple Sclerosis Society. His research is funded by the German Ministry for Education and Research (BMBF), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, Fresenius Foundation, the European Union, Hertie Foundation, NRW Ministry of Education and Research, Interdisciplinary Center for Clinical Studies (IZKF) Muenster and RE Children’s Foundation, Biogen, GlaxoSmithKline GmbH, Roche Pharma AG, and Sanofi-Genzyme. David Paling has participated as a speaker in meetings sponsored by, and received consulting fees from, Biogen, Celgene, Janssen, MedDay, Merck, Novartis, Sanofi Genzyme and Roche. Mitzi J. Williams has received consulting fees from EMD Serono, Horizon, Novartis, Alexion, Biogen, Sanofi, Genentech, Octave Biosciences, TG Therapeutics, Janssen, and Bristol Myers Squibb; and speaking fees from Genentech, Biogen, EMD Serono and TG Therapeutics. Ralf Gold has received compensation for serving as a consultant or speaker from Bayer HealthCare, Biogen Idec, Merck Serono, Novartis and Teva Neuroscience. He, or the institution he works for, has received research support from Bayer HealthCare, Biogen Idec, Merck Serono, Novartis and Teva Neuroscience. He has also received honoraria as a Journal Editor from SAGE and Thieme Verlag. Andrew Chan has received speakers’/board honoraria from Actelion (Janssen/J&J), Alexion, Almirall, Bayer, Biogen, Celgene (BMS), Merck KgaA, Novartis, Roche, Sanofi, and Teva, all for hospital research funds. He received research support from Biogen, Roche, Sanofi and UCB. Ron Milo has received research support from Bayer, Medison, Merck, Novartis and Teva; and honoraria or consulting fees from Actelion, Bayer, Biogen, Genzyme, Medison, Merck, Neopharm, Novartis, Roche, Sanofi, Teva and TG-Therapeutics. Patrick Vermersch has received honoraria and consulting fees from Biogen, Sanofi, Teva, Novartis, Merck, Imcyse, Roche and AB Science, and research support from Biogen, Sanofi and Merck. Ayan Das Gupta, Goeril Karlsson, Roseanne Sullivan, Gordon Graham, Martin Merschhemke and Dieter A. Häring are employees of Novartis.
Figures
References
-
- Hauser SL, Waubant E, Arnold DL, Vollmer T, Antel J, Fox RJ, et al. B-cell depletion with rituximab in relapsing-remitting multiple sclerosis. N Engl J Med. 2008;358(7):676–688. - PubMed
-
- Hauser SL, Bar-Or A, Comi G, Giovannoni G, Hartung HP, Hemmer B, et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. 2017;376(3):221–234. - PubMed
