

Dynamic susceptibility contrast perfusion-weighted and diffusion-weighted magnetic resonance imaging findings in pilocytic astrocytoma and H3.3 and H3.1 variant diffuse midline glioma, H3K27-altered
- PMID: 37450487
- PMCID: PMC10348548
- DOI: 10.1371/journal.pone.0288412
Dynamic susceptibility contrast perfusion-weighted and diffusion-weighted magnetic resonance imaging findings in pilocytic astrocytoma and H3.3 and H3.1 variant diffuse midline glioma, H3K27-altered
Abstract
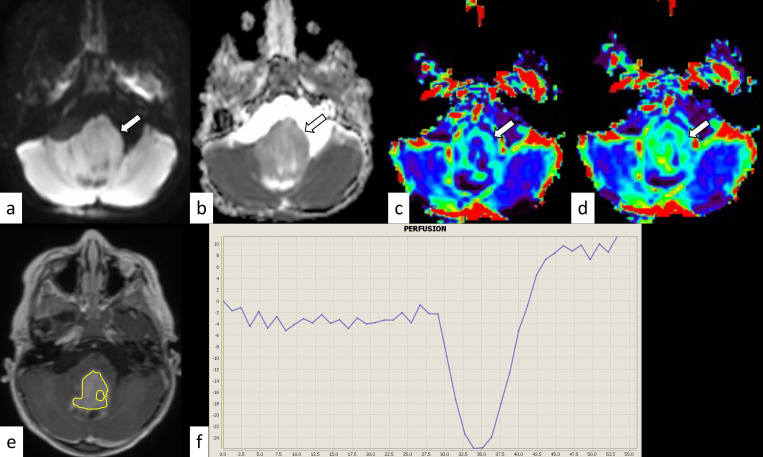
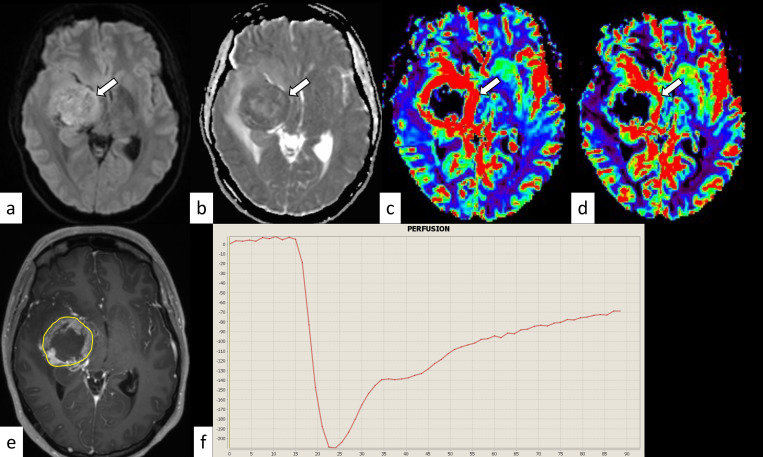
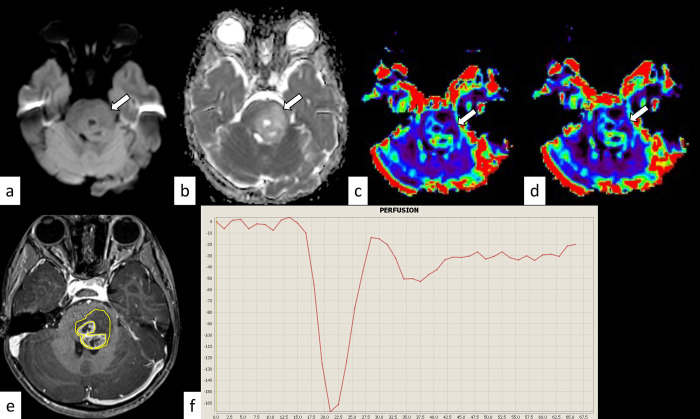
Objective: This study compared the dynamic susceptibility contrast (DSC) magnetic resonance imaging parameters and apparent diffusion coefficient (ADC) between pilocytic astrocytoma (PA) and diffuse midline glioma, H3K27-altered (DMG) variants.
Methods: The normalized relative cerebral blood volume (nrCBV), normalized relative flow (nrCBF), percentile signal recovery (PSR), and normalized mean ADC (nADCmean) of 23 patients with midline PAs (median age, 13 years [range, 1-71 years]; 13 female patients) and 40 patients with DMG (8.5 years [1-35 years]; 19 female patients), including 35 patients with H3.3- and five patients with H3.1-mutant tumors, treated between January 2016 and May 2022 were statistically compared.
Results: DMG had a significantly lower nADCmean (median: 1.48 vs. 1.96; p = 0.00075) and lower PSR (0.97 vs. 1.23, p = 0.13) but higher nrCBV and nrCBF (1.66 vs. 1.17, p = 0.058, respectively, and 1.87 vs. 1.19, p = 0.028, respectively) than PA. The H3.3 variant had a lower nADCmean than the H3.1 variant (1.46 vs. 1.80, p = 0.10).
Conclusion: DMG had lower ADC and PSR and higher rCBV and rCBF than PA. The H3.3 variant had a lower ADC than the H3.1 variant. Recognizing the differences and similarities in the DSC parameters and ADC between these tumors may help presurgical diagnosis.
Copyright: © 2023 Kurokawa et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
