

Predicting Long-term Disease-free Survival After Resection of Pancreatic Ductal Adenocarcinoma: A Nationwide Cohort Study
- PMID: 37450706
- PMCID: PMC10727199
- DOI: 10.1097/SLA.0000000000006004
Predicting Long-term Disease-free Survival After Resection of Pancreatic Ductal Adenocarcinoma: A Nationwide Cohort Study
Abstract
Objective: To develop a prediction model for long-term (≥5 years) disease-free survival (DFS) after the resection of pancreatic ductal adenocarcinoma (PDAC).
Background: Despite high recurrence rates, ~10% of patients have long-term DFS after PDAC resection. A model to predict long-term DFS may aid individualized prognostication and shared decision-making.
Methods: This nationwide cohort study included all consecutive patients who underwent PDAC resection in the Netherlands (2014-2016). The best-performing prognostic model was selected by Cox-proportional hazard analysis and Akaike's Information Criterion, presented by hazard ratios (HRs) with 95% confidence intervals (CIs). Internal validation was performed, and discrimination and calibration indices were assessed.
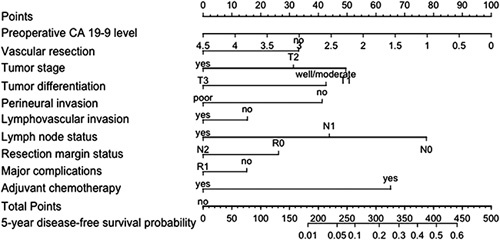
Results: In all, 836 patients with a median follow-up of 67 months (interquartile range 51-79) were analyzed. Long-term DFS was seen in 118 patients (14%). Factors predictive of long-term DFS were low preoperative carbohydrate antigen 19-9 (logarithmic; HR 1.21; 95% CI 1.10-1.32), no vascular resection (HR 1.33; 95% CI 1.12-1.58), T1 or T2 tumor stage (HR 1.52; 95% CI 1.14-2.04, and HR 1.17; 95% CI 0.98-1.39, respectively), well/moderate tumor differentiation (HR 1.44; 95% CI 1.22-1.68), absence of perineural and lymphovascular invasion (HR 1.42; 95% CI 1.11-1.81 and HR 1.14; 95% CI 0.96-1.36, respectively), N0 or N1 nodal status (HR 1.92; 95% CI 1.54-2.40, and HR 1.33; 95% CI 1.11-1.60, respectively), R0 resection margin status (HR 1.25; 95% CI 1.07-1.46), no major complications (HR 1.14; 95% CI 0.97-1.35) and adjuvant chemotherapy (HR 1.74; 95% CI 1.47-2.06). Moderate performance (concordance index 0.68) with adequate calibration (slope 0.99) was achieved.
Conclusions: The developed prediction model, readily available at www.pancreascalculator.com, can be used to estimate the probability of long-term DFS after resection of pancreatic ductal adenocarcinoma.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, et al. . Cancer Statistics, 2021. CA Cancer J Clin. 2021;71:7–33. - PubMed
-
- Neoptolemos JP, Stocken DD, Friess H, et al. . A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004;350:1200–1210. - PubMed
-
- Oettle H, Neuhaus P, Hochhaus A, et al. . Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA. 2013;310:1473–1481. - PubMed
-
- Conroy T, Hammel P, Hebbar M, et al. . FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. 2018;379:2395–2406. - PubMed
-
- Shibata K, Matsumoto T, Yada K, et al. . Factors predicting recurrence after resection of pancreatic ductal carcinoma. Pancreas. 2005;31:69–73. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
