

Pulmonary Hypertension: A Contemporary Review
- PMID: 37450768
- PMCID: PMC10492255
- DOI: 10.1164/rccm.202302-0327SO
Pulmonary Hypertension: A Contemporary Review
Abstract
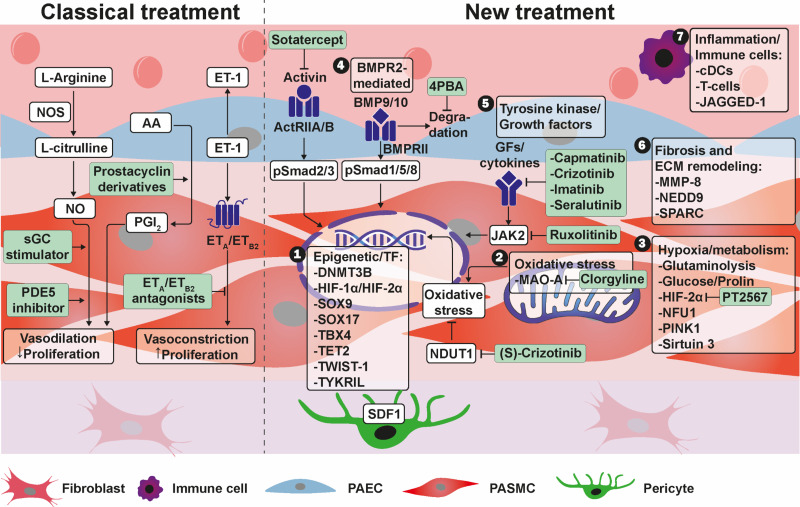
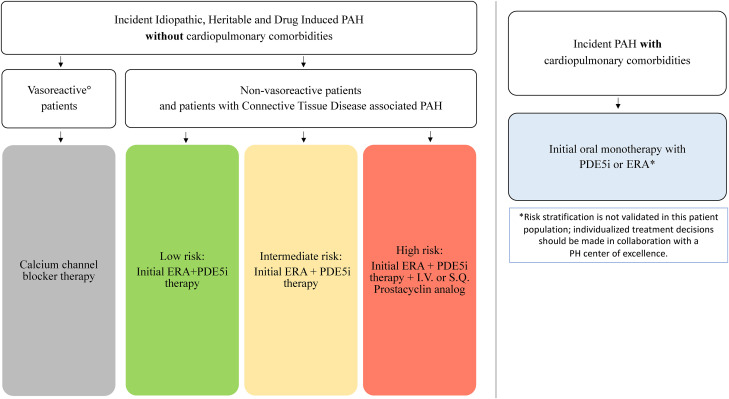
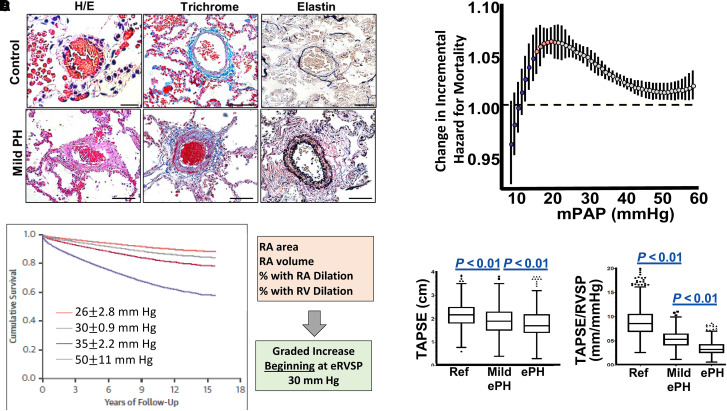
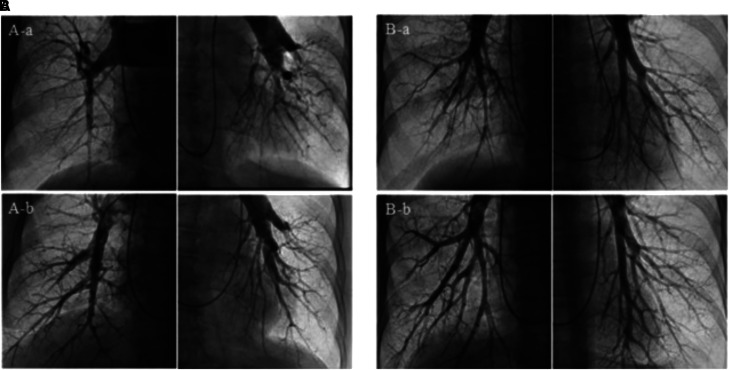
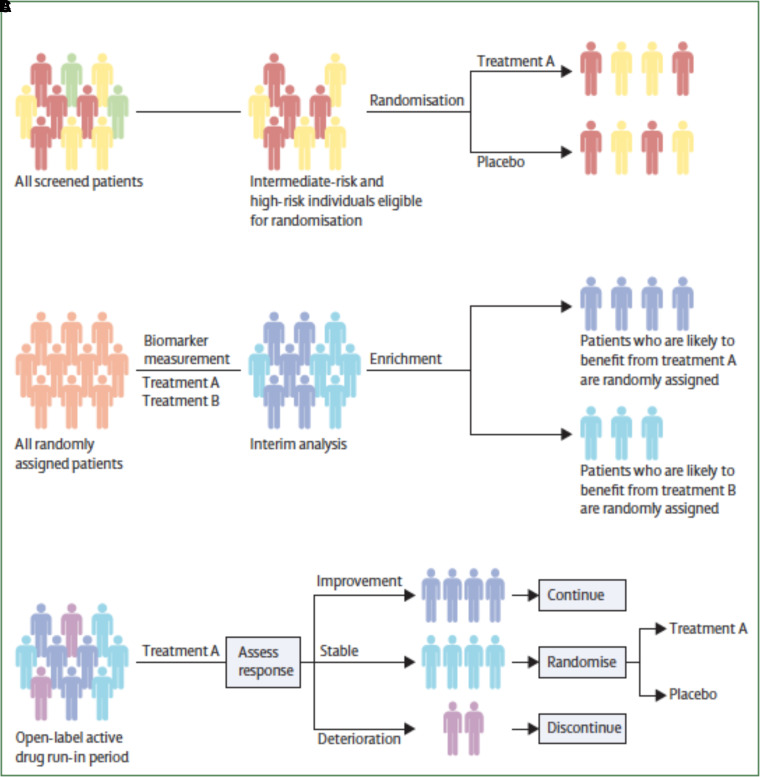
Major advances in pulmonary arterial hypertension, pulmonary hypertension (PH) associated with lung disease, and chronic thromboembolic PH cast new light on the pathogenetic mechanisms, epidemiology, diagnostic approach, and therapeutic armamentarium for pulmonary vascular disease. Here, we summarize key basic, translational, and clinical PH reports, emphasizing findings that build on current state-of-the-art research. This review includes cutting-edge progress in translational pulmonary vascular biology, with a guide to the diagnosis of patients in clinical practice, incorporating recent PH definition revisions that continue emphasis on early detection of disease. PH management is reviewed including an overview of the evolving considerations for the approach to treatment of PH in patients with cardiopulmonary comorbidities, as well as a discussion of the groundbreaking sotatercept data for the treatment of pulmonary arterial hypertension.
Keywords: pulmonary arterial hypertension; pulmonary hypertension; pulmonary vascular disease.
Figures
Comment in
-
Let's Talk About Respiratory Swings!Am J Respir Crit Care Med. 2023 Dec 15;208(12):1338-1340. doi: 10.1164/rccm.202309-1637LE. Am J Respir Crit Care Med. 2023. PMID: 37871311 Free PMC article. No abstract available.
References
-
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. ESC/ERS Scientific Document Group 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J . 2022;43:3618–3731. - PubMed
-
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J . 2023;61:2200879. - PubMed
-
- Humbert M, McLaughlin V, Gibbs JSR, Gomberg-Maitland M, Hoeper MM, Preston IR, et al. PULSAR Trial Investigators Sotatercept for the treatment of pulmonary arterial hypertension. N Engl J Med . 2021;384:1204–1215. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
