

A Double-Blind, Randomized, Placebo-controlled Trial of Long-Term Doxycycline Therapy on Exacerbation Rate in Patients with Stable Chronic Obstructive Pulmonary Disease
- PMID: 37450935
- PMCID: PMC10492249
- DOI: 10.1164/rccm.202212-2287OC
A Double-Blind, Randomized, Placebo-controlled Trial of Long-Term Doxycycline Therapy on Exacerbation Rate in Patients with Stable Chronic Obstructive Pulmonary Disease
Abstract
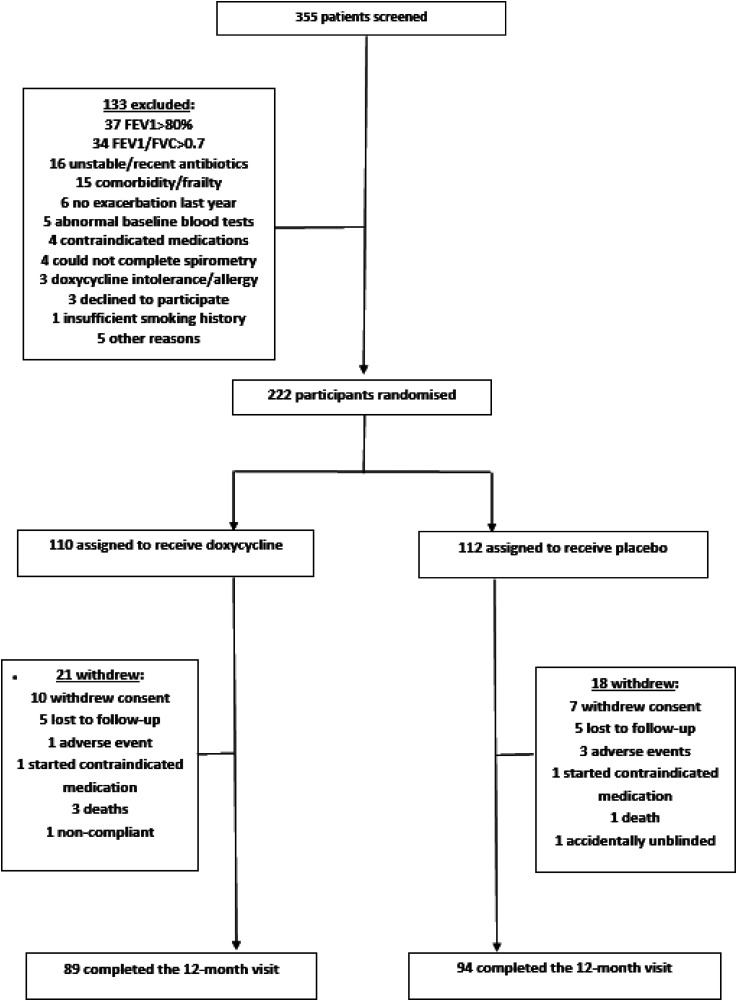
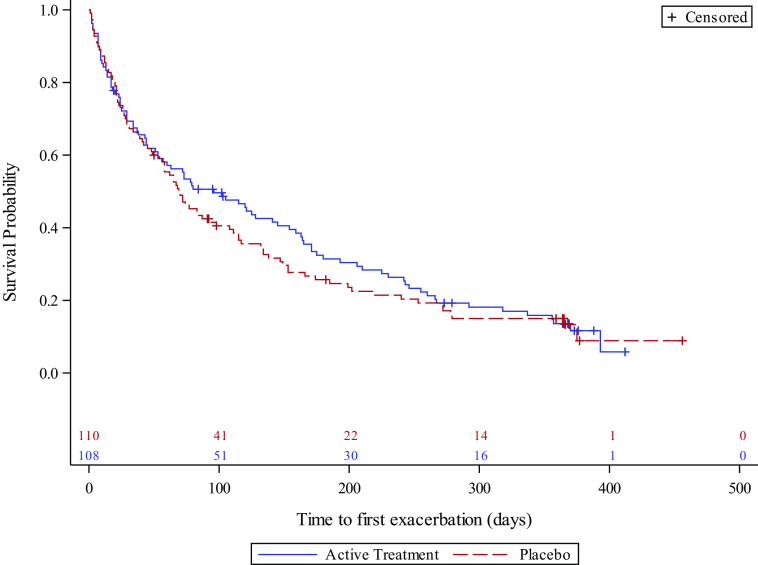
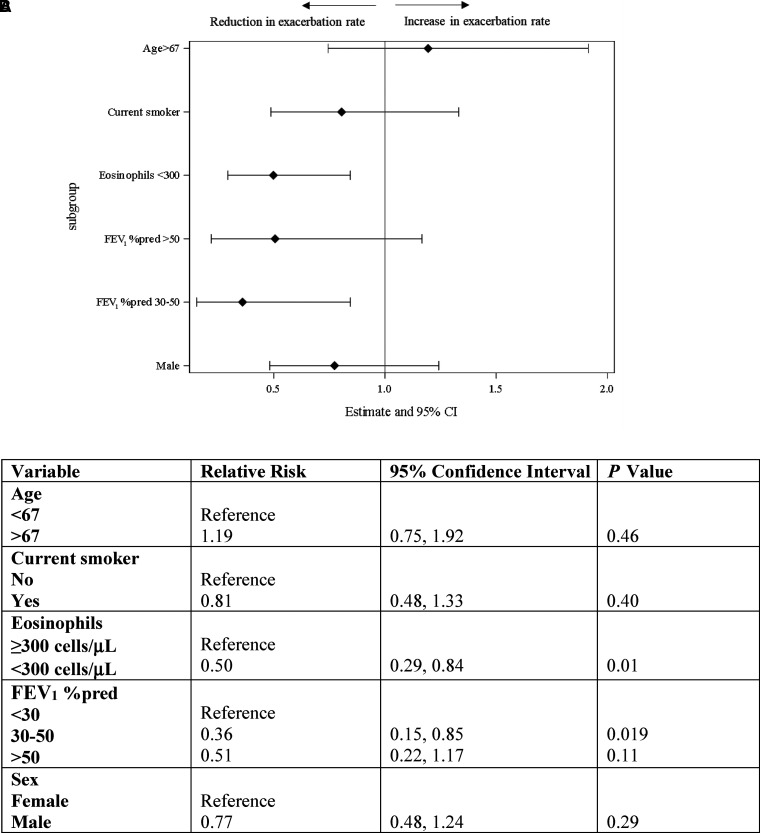
Rationale: Chronic obstructive pulmonary disease (COPD) exacerbations are a major cause of morbidity and mortality, and preventing them is a key treatment target. Long-term macrolide treatment is effective at reducing exacerbations, but there is a paucity of evidence for other antibiotic classes. Objectives: To assess whether 12-month use of doxycycline reduces the exacerbation rate in people with COPD. Methods: People with moderate to very severe COPD and an exacerbation history were recruited from three UK centers and randomized to 12 months of doxycycline 100 mg once daily or placebo. The primary study outcome was the exacerbation rate per person-year. Results: A total of 222 people were randomized. Baseline mean FEV1 was 1.35 L (SD, 0.35 L), 52.5% predicted (SD, 15.9% predicted). The median number of treated exacerbations in the year before the study was 2 (SD, 1-4). A total of 71% of patients reported two or more exacerbations, and 81% were already prescribed inhaled corticosteroids at baseline. The COPD exacerbation rate did not differ between the groups (doxycycline/placebo rate ratio [RR], 0.86; 95% confidence interval [CI], 0.67-1.10; P = 0.23). No difference was seen if only treated exacerbations or hospitalizations were considered. In preplanned subgroup analysis, doxycycline appeared to better reduce the exacerbation rate among people with severe COPD (RR, 0.36; 95% CI, 0.15-0.85; P = 0.019) and in those with an eosinophil count <300 cells/μl (RR, 0.50; 95% CI, 0.29-0.84; P = 0.01). Health status measured by St. George's Respiratory Questionnaire was 5.2 points worse in the doxycycline group at 12 months (P < 0.007). Conclusions: Doxycycline did not significantly reduce the exacerbation rate, over 12 months, in participants with COPD who exacerbated regularly, but it may have benefitted those with more severe COPD or blood eosinophil counts <300 cells/μl. Clinical trial registered with www.clinicaltrials.gov (NCT02305940).
Keywords: antibiotic; chronic obstructive pulmonary disease; clinical trial; exacerbations; long-term.
Figures
Comment in
-
Revisiting the Use of Antibiotics to Prevent COPD Exacerbation: Is Doxycycline the Answer?Am J Respir Crit Care Med. 2023 Sep 1;208(5):509-511. doi: 10.1164/rccm.202307-1302ED. Am J Respir Crit Care Med. 2023. PMID: 37531185 Free PMC article. No abstract available.
-
Microbiological Monitoring in Therapeutic Trials in Chronic Obstructive Pulmonary Disease.Am J Respir Crit Care Med. 2023 Nov 15;208(10):1142-1143. doi: 10.1164/rccm.202307-1214LE. Am J Respir Crit Care Med. 2023. PMID: 37734068 Free PMC article. No abstract available.
-
Long-Term Doxycycline Therapy for Stable Chronic Obstructive Pulmonary Disease: Do the Benefits Outweigh the Drawbacks?Am J Respir Crit Care Med. 2023 Nov 15;208(10):1143-1144. doi: 10.1164/rccm.202307-1301LE. Am J Respir Crit Care Med. 2023. PMID: 37734069 Free PMC article. No abstract available.
References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med . 2017;195:557–582. - PubMed
-
- Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med . 1998;157:1418–1422. - PubMed
-
- National Clinical Guideline Centre. 2018. https://www.nice.org.uk/guidance/ng115
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
