

Genetics of diabetes-associated microvascular complications
- PMID: 37452207
- PMCID: PMC10390394
- DOI: 10.1007/s00125-023-05964-x
Genetics of diabetes-associated microvascular complications
Abstract
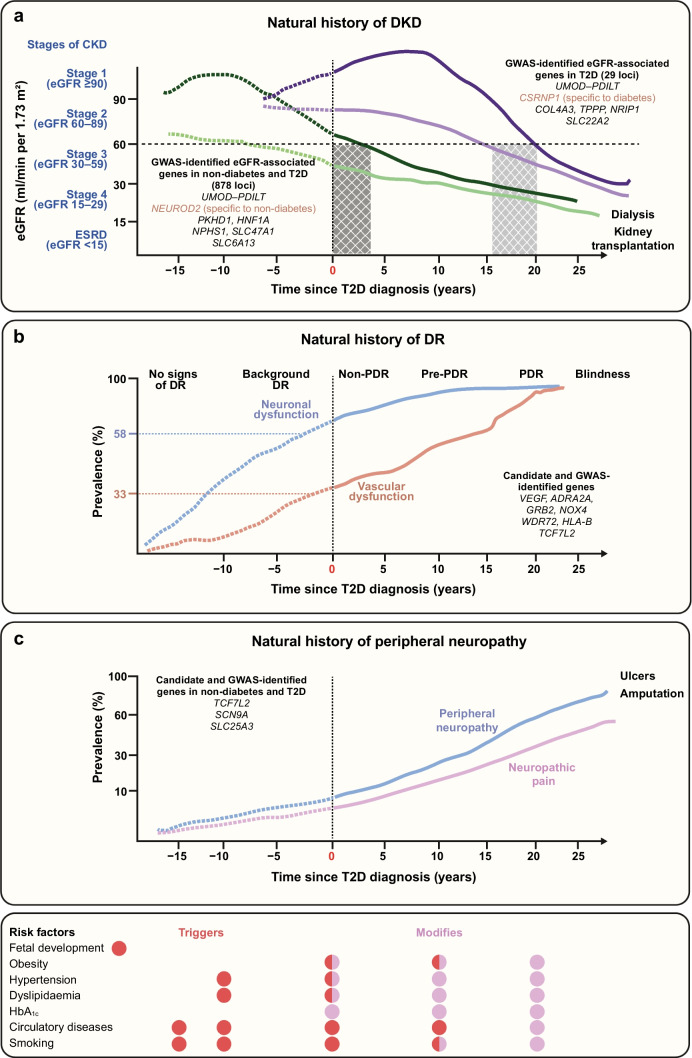
Diabetes is associated with excess morbidity and mortality due to both micro- and macrovascular complications, as well as a range of non-classical comorbidities. Diabetes-associated microvascular complications are those considered most closely related to hyperglycaemia in a causal manner. However, some individuals with hyperglycaemia (even those with severe hyperglycaemia) do not develop microvascular diseases, which, together with evidence of co-occurrence of microvascular diseases in families, suggests a role for genetics. While genome-wide association studies (GWASs) produced firm evidence of multiple genetic variants underlying differential susceptibility to type 1 and type 2 diabetes, genetic determinants of microvascular complications are mostly suggestive. Identified susceptibility variants of diabetic kidney disease (DKD) in type 2 diabetes mirror variants underlying chronic kidney disease (CKD) in individuals without diabetes. As for retinopathy and neuropathy, reported risk variants currently lack large-scale replication. The reported associations between type 2 diabetes risk variants and microvascular complications may be explained by hyperglycaemia. More extensive phenotyping, along with adjustments for unmeasured confounding, including both early (fetal) and late-life (hyperglycaemia, hypertension, etc.) environmental factors, are urgently needed to understand the genetics of microvascular complications. Finally, genetic variants associated with reduced glycolysis, mitochondrial dysfunction and DNA damage and sustained cell regeneration may protect against microvascular complications, illustrating the utility of studies in individuals who have escaped these complications.
Keywords: DNA; Diabetes; Genetics; Intrauterine programming; Metabolism; Microvascular diseases; Nephropathy; Neuropathy; Retinopathy; Review.
© 2023. The Author(s).
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
