

Diagnostic management of acute pulmonary embolism: a prediction model based on a patient data meta-analysis
- PMID: 37452732
- PMCID: PMC10917087
- DOI: 10.1093/eurheartj/ehad417
Diagnostic management of acute pulmonary embolism: a prediction model based on a patient data meta-analysis
Abstract
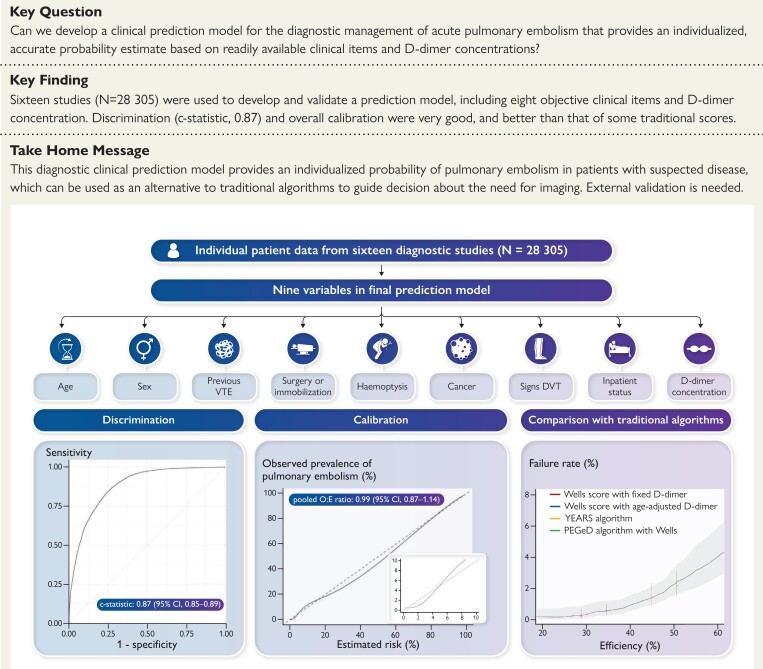
Aims: Risk stratification is used for decisions regarding need for imaging in patients with clinically suspected acute pulmonary embolism (PE). The aim was to develop a clinical prediction model that provides an individualized, accurate probability estimate for the presence of acute PE in patients with suspected disease based on readily available clinical items and D-dimer concentrations.
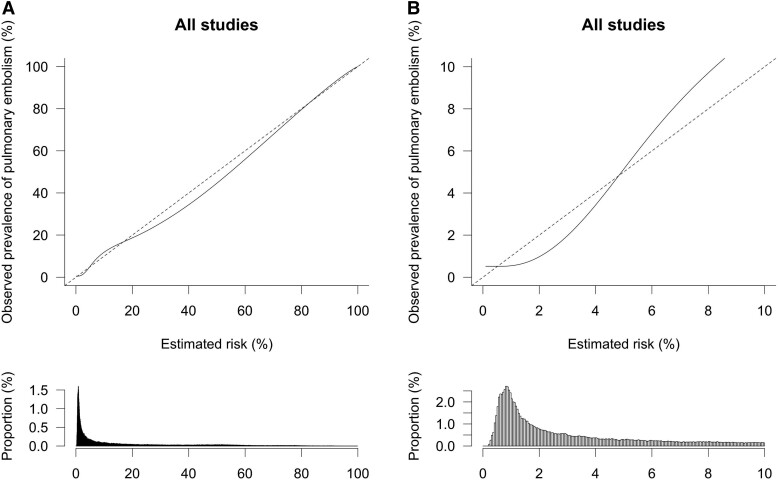
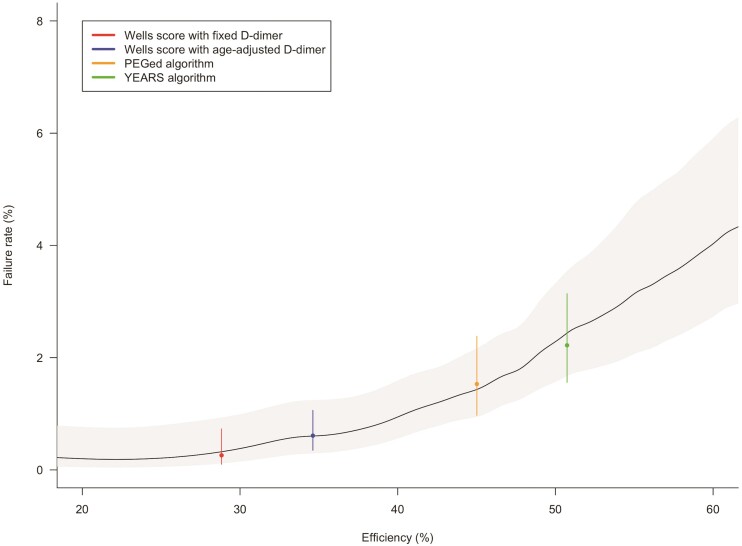
Methods and results: An individual patient data meta-analysis was performed based on sixteen cross-sectional or prospective studies with data from 28 305 adult patients with clinically suspected PE from various clinical settings, including primary care, emergency care, hospitalized and nursing home patients. A multilevel logistic regression model was built and validated including ten a priori defined objective candidate predictors to predict objectively confirmed PE at baseline or venous thromboembolism (VTE) during follow-up of 30 to 90 days. Multiple imputation was used for missing data. Backward elimination was performed with a P-value <0.10. Discrimination (c-statistic with 95% confidence intervals [CI] and prediction intervals [PI]) and calibration (outcome:expected [O:E] ratio and calibration plot) were evaluated based on internal-external cross-validation. The accuracy of the model was subsequently compared with algorithms based on the Wells score and D-dimer testing. The final model included age (in years), sex, previous VTE, recent surgery or immobilization, haemoptysis, cancer, clinical signs of deep vein thrombosis, inpatient status, D-dimer (in µg/L), and an interaction term between age and D-dimer. The pooled c-statistic was 0.87 (95% CI, 0.85-0.89; 95% PI, 0.77-0.93) and overall calibration was very good (pooled O:E ratio, 0.99; 95% CI, 0.87-1.14; 95% PI, 0.55-1.79). The model slightly overestimated VTE probability in the lower range of estimated probabilities. Discrimination of the current model in the validation data sets was better than that of the Wells score combined with a D-dimer threshold based on age (c-statistic 0.73; 95% CI, 0.70-0.75) or structured clinical pretest probability (c-statistic 0.79; 95% CI, 0.76-0.81).
Conclusion: The present model provides an absolute, individualized probability of PE presence in a broad population of patients with suspected PE, with very good discrimination and calibration. Its clinical utility needs to be evaluated in a prospective management or impact study.
Registration: PROSPERO ID 89366.
Keywords: D-dimer; Pulmonary embolism; diagnosis; prediction model; venous thromboembolism.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
A novel prediction model for pulmonary embolism: from dichotomizing algorithms to personalized likelihood.Eur Heart J. 2023 Aug 22;44(32):3082-3084. doi: 10.1093/eurheartj/ehad392. Eur Heart J. 2023. PMID: 37475706 No abstract available.
References
-
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). Eur Heart J 2020;41:543–603. 10.1093/eurheartj/ehz405 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
