

Artificial intelligence in detecting left atrial appendage thrombus by transthoracic echocardiography and clinical features: the Left Atrial Thrombus on Transoesophageal Echocardiography (LATTEE) registry
- PMID: 37453044
- PMCID: PMC10757867
- DOI: 10.1093/eurheartj/ehad431
Artificial intelligence in detecting left atrial appendage thrombus by transthoracic echocardiography and clinical features: the Left Atrial Thrombus on Transoesophageal Echocardiography (LATTEE) registry
Abstract
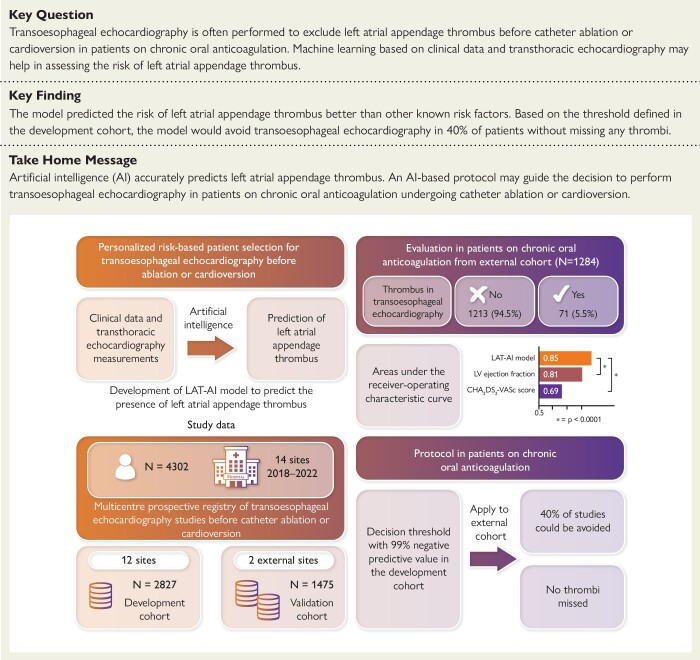
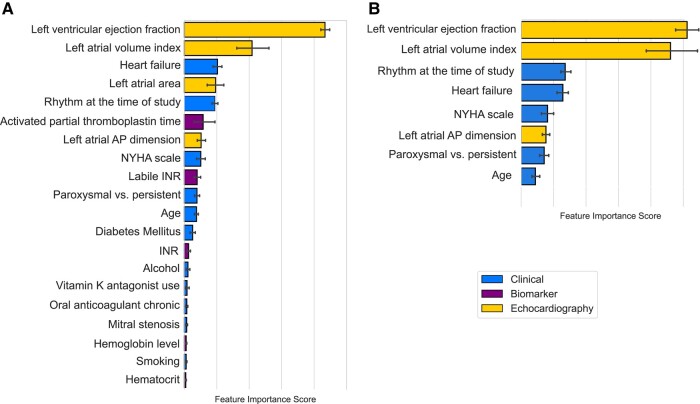
Aims: Transoesophageal echocardiography (TOE) is often performed before catheter ablation or cardioversion to rule out the presence of left atrial appendage thrombus (LAT) in patients on chronic oral anticoagulation (OAC), despite associated discomfort. A machine learning model [LAT-artificial intelligence (AI)] was developed to predict the presence of LAT based on clinical and transthoracic echocardiography (TTE) features.
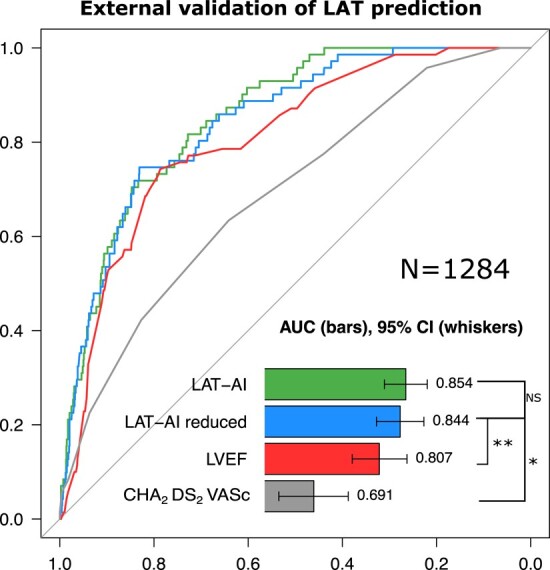
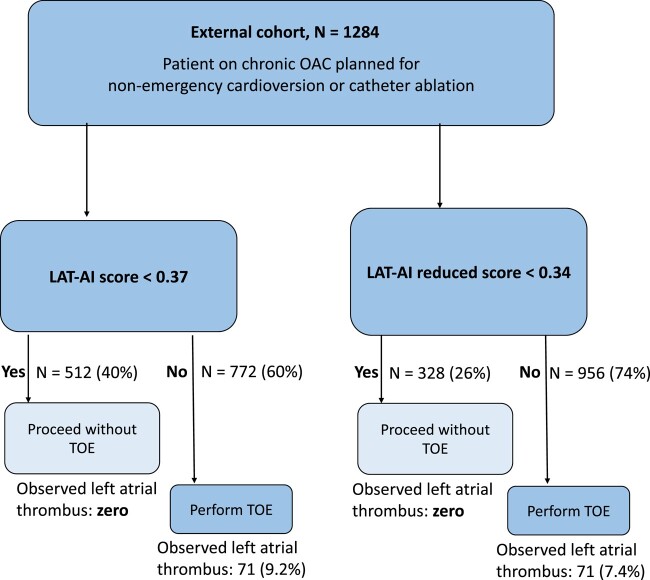
Methods and results: Data from a 13-site prospective registry of patients who underwent TOE before cardioversion or catheter ablation were used. LAT-AI was trained to predict LAT using data from 12 sites (n = 2827) and tested externally in patients on chronic OAC from two sites (n = 1284). Areas under the receiver operating characteristic curve (AUC) of LAT-AI were compared with that of left ventricular ejection fraction (LVEF) and CHA2DS2-VASc score. A decision threshold allowing for a 99% negative predictive value was defined in the development cohort. A protocol where TOE in patients on chronic OAC is performed depending on the LAT-AI score was validated in the external cohort. In the external testing cohort, LAT was found in 5.5% of patients. LAT-AI achieved an AUC of 0.85 [95% confidence interval (CI): 0.82-0.89], outperforming LVEF (0.81, 95% CI 0.76-0.86, P < .0001) and CHA2DS2-VASc score (0.69, 95% CI: 0.63-0.7, P < .0001) in the entire external cohort. Based on the proposed protocol, 40% of patients on chronic OAC from the external cohort would safely avoid TOE.
Conclusion: LAT-AI allows accurate prediction of LAT. A LAT-AI-based protocol could be used to guide the decision to perform TOE despite chronic OAC.
Keywords: Ablation • Cardioversion • Left atrial appendage thrombus • Machine learning.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Artificial intelligence and innovation of clinical care: the need for evidence in the real world.Eur Heart J. 2024 Jan 1;45(1):42-44. doi: 10.1093/eurheartj/ehad553. Eur Heart J. 2024. PMID: 37670406 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
