

Real-world assessment of immunogenicity in immunocompromised individuals following SARS-CoV-2 mRNA vaccination: a one-year follow-up of the prospective clinical trial COVAXID
- PMID: 37453361
- PMCID: PMC10365982
- DOI: 10.1016/j.ebiom.2023.104700
Real-world assessment of immunogenicity in immunocompromised individuals following SARS-CoV-2 mRNA vaccination: a one-year follow-up of the prospective clinical trial COVAXID
Abstract
Background: Immunocompromised patients have varying responses to SARS-CoV-2 mRNA vaccination. However, there is limited information available from prospective clinical trial cohorts with respect to long-term immunogenicity-related responses in these patient groups following three or four vaccine doses, and in applicable cases infection.
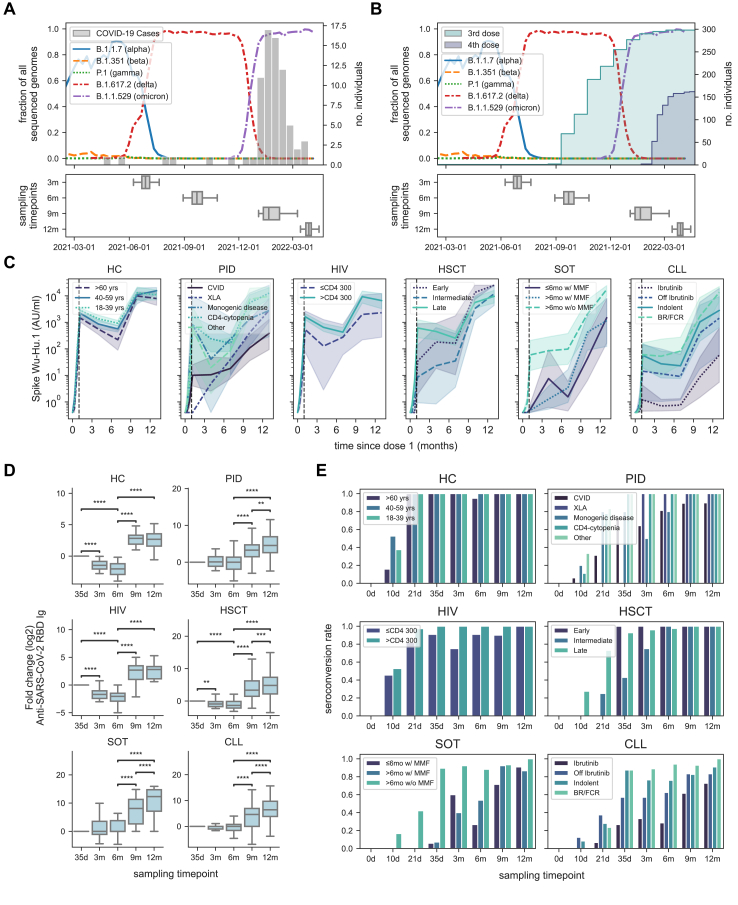
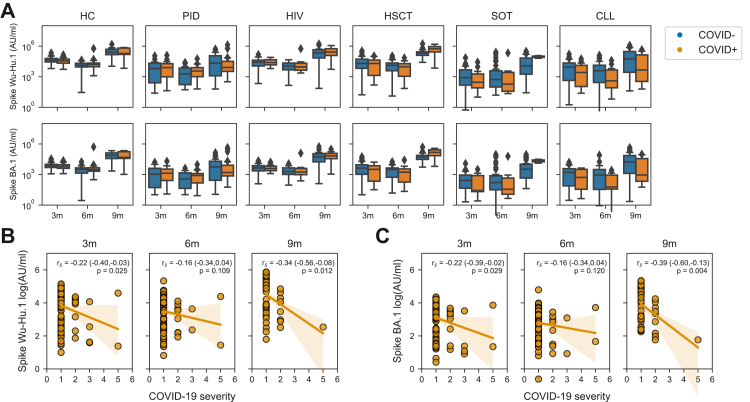
Methods: In a real-world setting, we assessed the long-term immunogenicity-related responses in patients with primary and secondary immunodeficiencies from the prospective open-label clinical trial COVAXID. The original clinical trial protocol included two vaccine doses given on days 0 and 21, with antibody titres measured at six different timepoints over six months. The study cohort has subsequently been followed for one year with antibody responses evaluated in relation to the third and fourth vaccine dose, and in applicable cases SARS-CoV-2 infection. In total 356/539 patients were included in the extended cohort. Blood samples were analysed for binding antibody titres and neutralisation against the Spike protein for all SARS-CoV-2 variants prevailing during the study period, including Omicron subvariants. SARS-CoV-2 infections that did not require hospital care were recorded through quarterly in-person, or phone-, interviews and assessment of IgG antibody titres against SARS-CoV-2 Nucleocapsid. The original clinical trial was registered in EudraCT (2021-000175-37) and clinicaltrials.gov (NCT04780659).
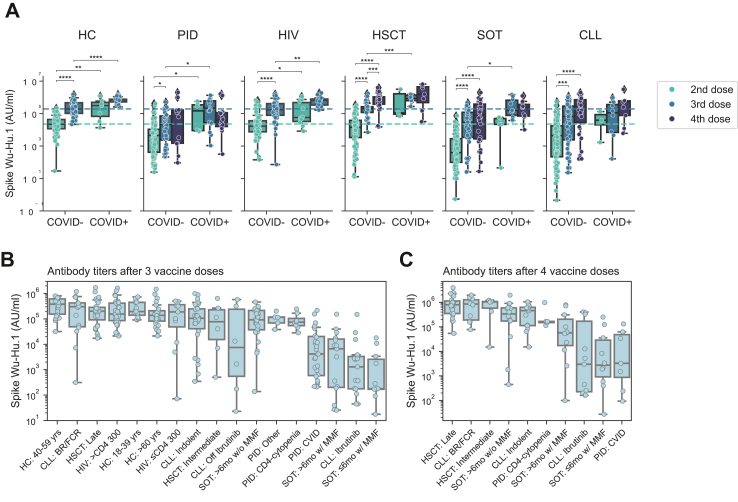
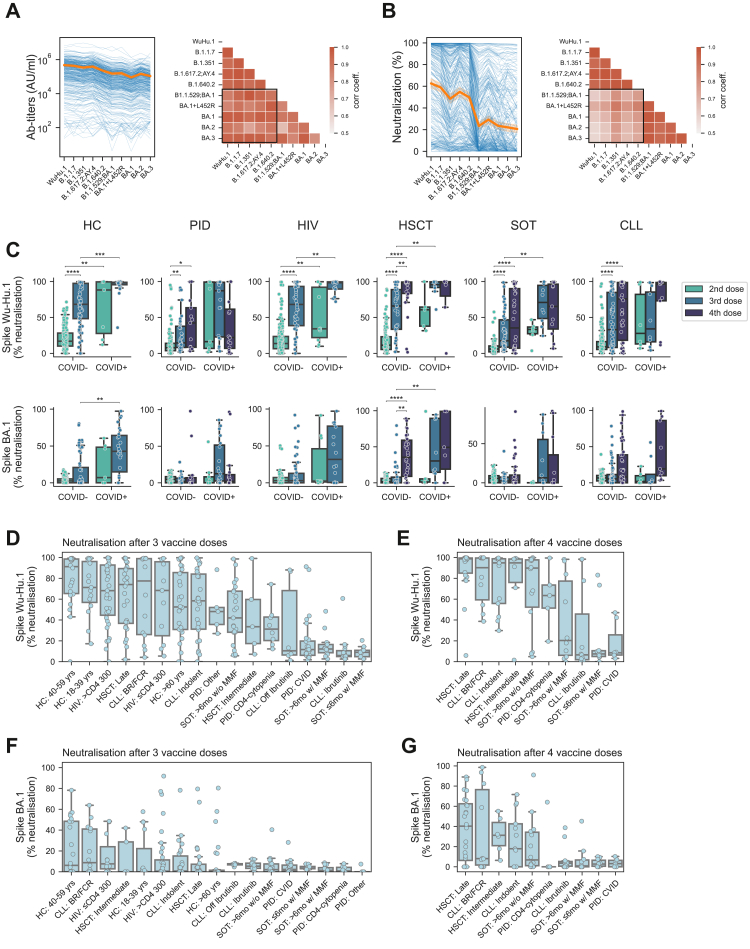
Findings: The third vaccine dose significantly increased Spike IgG titres against all the SARS-CoV-2 variants analysed in all immunocompromised patient groups. Similarly, neutralisation also increased against all variants studied, except for Omicron. Omicron-specific neutralisation, however, increased after a fourth dose as well as after three doses and infection in many of the patient subgroups. Noteworthy, however, while many patient groups mounted strong serological responses after three and four vaccine doses, comparably weak responders were found among patient subgroups with specific primary immunodeficiencies and subgroups with immunosuppressive medication.
Interpretation: The study identifies particularly affected patient groups in terms of development of long-term immunity among a larger group of immunocompromised patients. In particular, the results highlight poor vaccine-elicited neutralising responses towards Omicron subvariants in specific subgroups. The results provide additional knowledge of relevance for future vaccination strategies.
Funding: The present studies were supported by grants from the Swedish Research Council, the Knut and Alice Wallenberg Foundation, Nordstjernan AB, Region Stockholm, and Karolinska Institutet.
Keywords: COVID-19; Chronic lymphocytic leukemia; Clinical study; HIV; Haematopoietic stem cell transplantation; Primary immunodeficiency disease; SARS-CoV-2; Solid organ transplantation; mRNA vaccine.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests PB has received honoraria from Takeda for educational lectures not directly relevant to this work. SM has received honoraria from Celgene/BMS, Novartis, Gilead/Kite, DNA Prime for lectures and educational events and as a member and/or head of data safety monitoring boards from Miltenyi and Immunicum not directly relevant to this work. CIES has received financial support from Moderna for work not directly relevant to this work. KL has received financial support from Moderna for work not directly relevant to this work. PL has received grants from Pfizer, MSD, and personal fees from Takeda, AiCuris, and OctaPharma, not directly relevant to the submitted work. SA has received honoraria for lectures and educational events, from Gilead, AbbVie, MSD, Biogen and Netdoktor, not directly related to this work, and reports grants from the Swedish Research Council on COVID-19 vaccination. HGL received honoraria from Sanofi for consultation not relevant to this work, and has served on the UK-CIC Oversight Committee, had led the Karolinska Institutet COVID-19 vaccine group, and is on the scientific advisory group for the International Vaccine Institute not directly relevant to this work, and reports grants from Knut and Alice Wallenberg Foundation, Nordstjernan AB, Region Stockholm, and Karolinska Institutet for studies on COVID-19 and COVID-19 vaccination. All other authors declare no potential or actual conflict of interest to the work presented in this paper.
Figures
References
-
- Mahase E. Covid-19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ. 2020;368:m1036. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
