

Guided implantation of a leadless left ventricular endocardial electrode and acoustic transmitter using computed tomography anatomy, dynamic perfusion and mechanics, and predicted activation pattern
- PMID: 37453603
- PMCID: PMC10850882
- DOI: 10.1016/j.hrthm.2023.07.007
Guided implantation of a leadless left ventricular endocardial electrode and acoustic transmitter using computed tomography anatomy, dynamic perfusion and mechanics, and predicted activation pattern
Abstract
Background: The WiSE-CRT System (EBR systems, Sunnyvale, CA) permits leadless left ventricular pacing. Currently, no intraprocedural guidance is used to target optimal electrode placement while simultaneously guiding acoustic transmitter placement in close proximity to the electrode to ensure adequate power delivery.
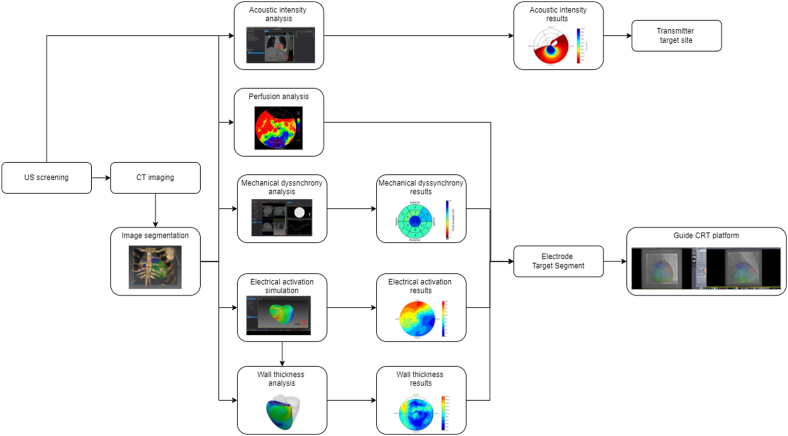
Objective: The purpose of this study was to assess the use of computed tomography (CT) anatomy, dynamic perfusion and mechanics, and predicted activation pattern to identify both the optimal electrode and transmitter locations.
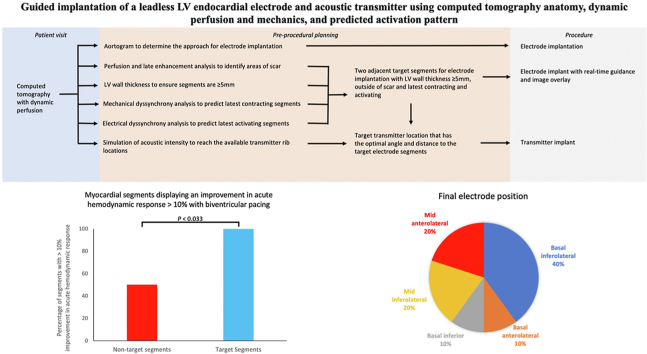
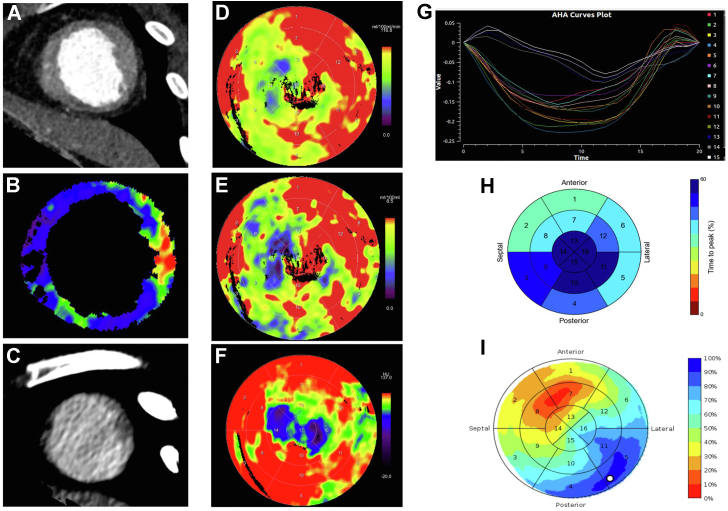
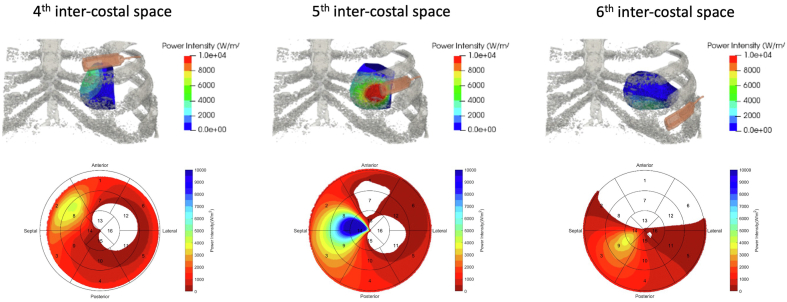
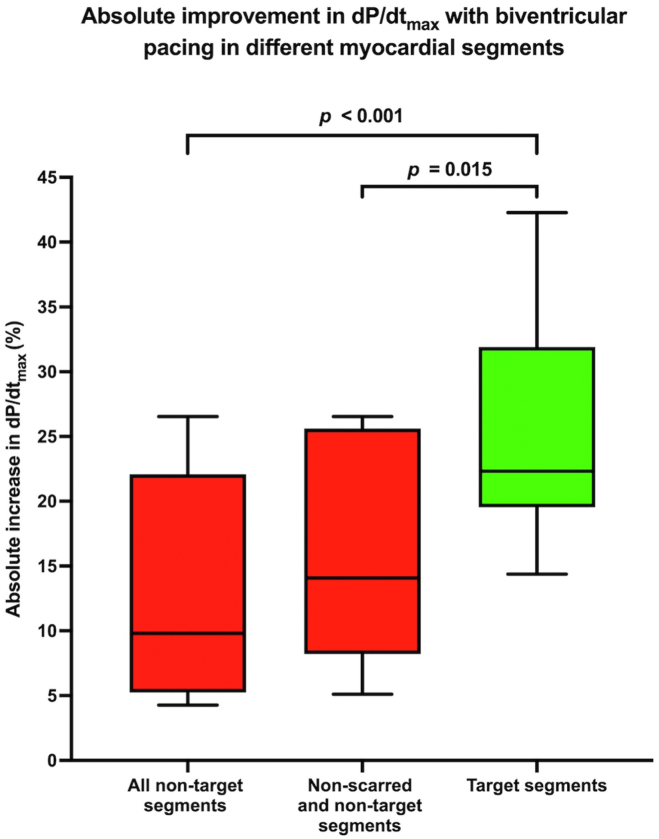
Methods: A novel CT protocol was developed using preprocedural imaging and simulation to identify target segments (TSs) for electrode implantation, with late electrical and mechanical activation, with ≥5 mm wall thickness without perfusion defects. Modeling of the acoustic intensity from different transmitter implantation sites to the TSs was used to identify the optimal transmitter location. During implantation, TSs were overlaid on fluoroscopy to guide optimal electrode location that were evaluated by acute hemodynamic response (AHR) by measuring the maximal rate of left ventricular pressure rise with biventricular pacing.
Results: Ten patients underwent the implantation procedure. The transmitter could be implanted within the recommended site on the basis of preprocedural analysis in all patients. CT identified a mean of 4.8 ± 3.5 segments per patient with wall thickness < 5 mm. During electrode implantation, biventricular pacing within TSs resulted in a significant improvement in AHR vs non-TSs (25.5% ± 8.8% vs 12.9% ± 8.6%; P < .001). Pacing in CT-identified scar resulted in either failure to capture or minimal AHR improvement. The electrode was targeted to the TSs in all patients and was implanted in the TSs in 80%.
Conclusion: Preprocedural imaging and modeling data with intraprocedural guidance can successfully guide WiSE-CRT electrode and transmitter implantation to allow optimal AHR and adequate power delivery.
Keywords: Cardiac resynchronization therapy; Endocardial pacing; Guiding endocardial pacing; Hemodynamic assessment; WiSE-CRT.
Copyright © 2023 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Sieniewicz B.J., Behar J.M., Gould J., et al. Guidance for optimal site selection of a leadless left ventricular endocardial electrode improves acute hemodynamic response and chronic remodeling. JACC Clin Electrophysiol. 2018;4:860–868. - PubMed
-
- DeFaria Yeh D., Lonergan K.L., Fu D., Yeh R.W., Echt D.S., Foster E. Clinical factors and echocardiographic techniques related to the presence, size, and location of acoustic windows for leadless cardiac pacing. Europace. 2011;13:1760–1765. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
