

Impaired in vitro fertilization outcomes following testosterone treatment improve with washout in a mouse model of gender-affirming hormone treatment
- PMID: 37453652
- PMCID: PMC10654792
- DOI: 10.1016/j.ajog.2023.07.013
Impaired in vitro fertilization outcomes following testosterone treatment improve with washout in a mouse model of gender-affirming hormone treatment
Abstract
Background: The impact of gender-affirming testosterone on fertility is poorly understood, with ovarian histopathologic studies showing variable results, some with a detrimental effect on reproductive capacity and uncertain reversibility. Assisted reproductive outcome data are restricted to small case series that lack the ability to inform clinical practice guidelines and limit fertility preservation counseling for transgender and nonbinary individuals.
Objective: This study aimed to determine the impact of current testosterone and testosterone washout on in vitro fertilization outcomes in a mouse model for gender-affirming hormone treatment. We hypothesized that current or previous testosterone treatment would not affect in vitro fertilization outcomes.
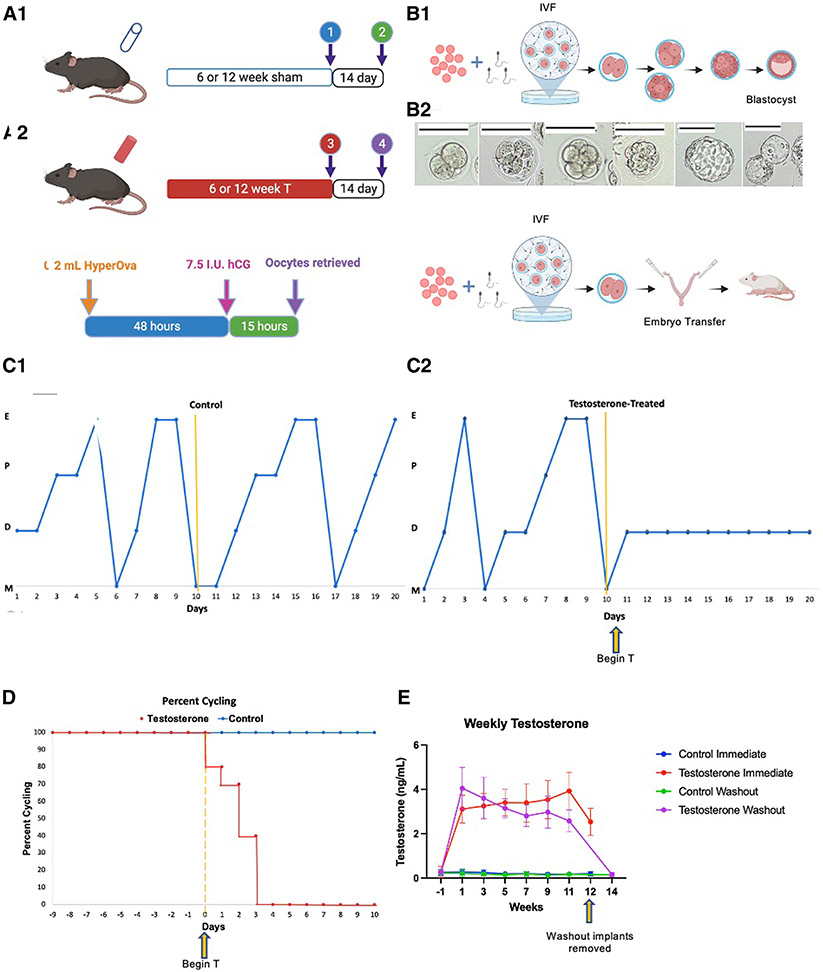
Study design: C57BL/6N female mice (n=120) were assigned to 4 treatment groups: (1) current control, (2) current testosterone, (3) control washout, and (4) testosterone washout. Testosterone implants remained in situ for 6 or 12 weeks, representing the short- and long-term treatment arms, respectively. Current treatment groups underwent ovarian stimulation with implants in place, and washout treatment groups were explanted and had ovarian stimulation after 2 weeks. Oocytes were collected, fertilized, and cultured in vitro, with one arm continuing to the blastocyst stage and the other having transfer of cleavage-stage embryos. Statistical analysis was performed using GraphPad Prism, version 9.0 and R statistical software, version 4.1.2, with statistical significance defined by P<.05.
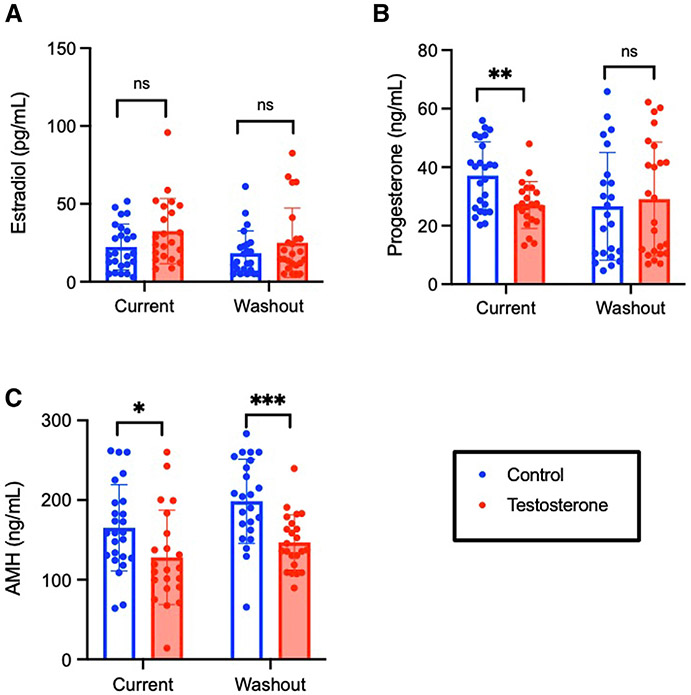
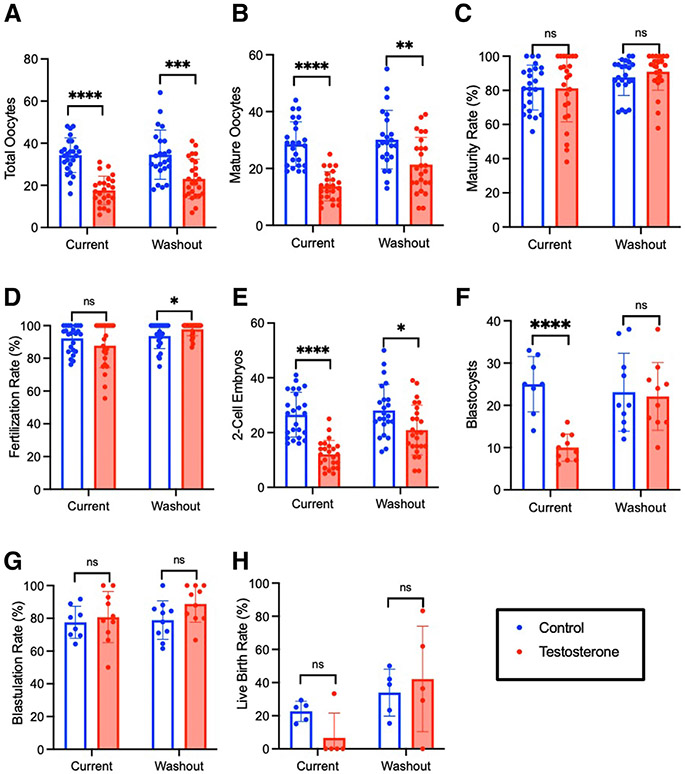
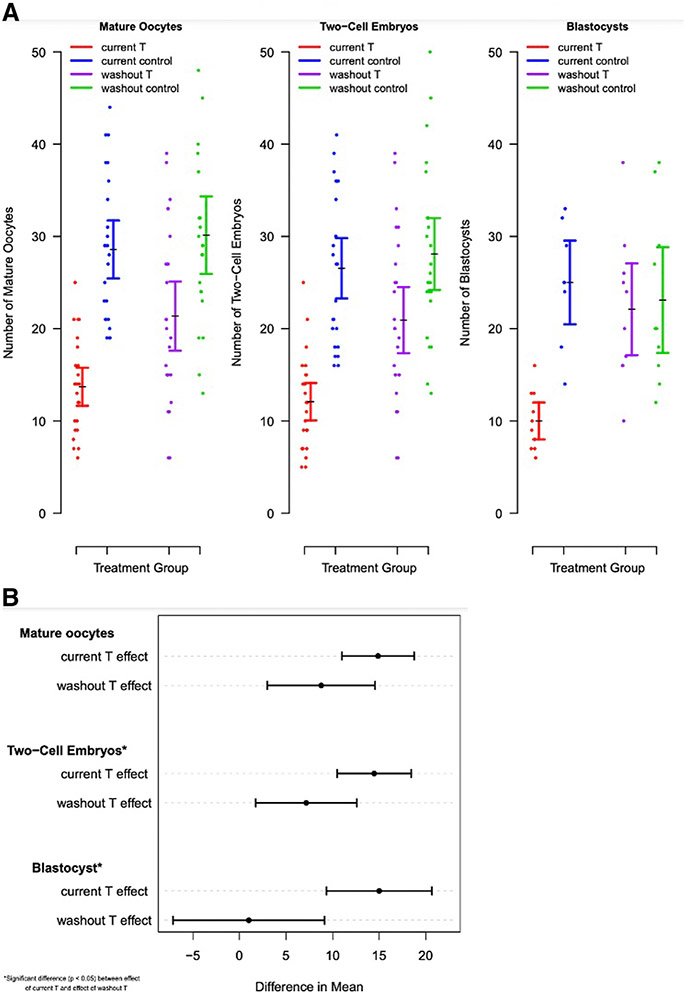
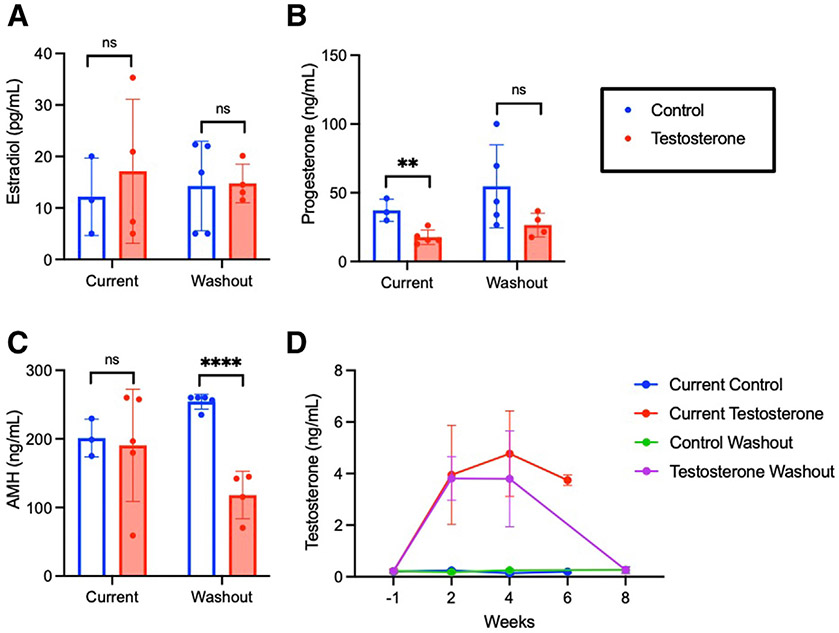
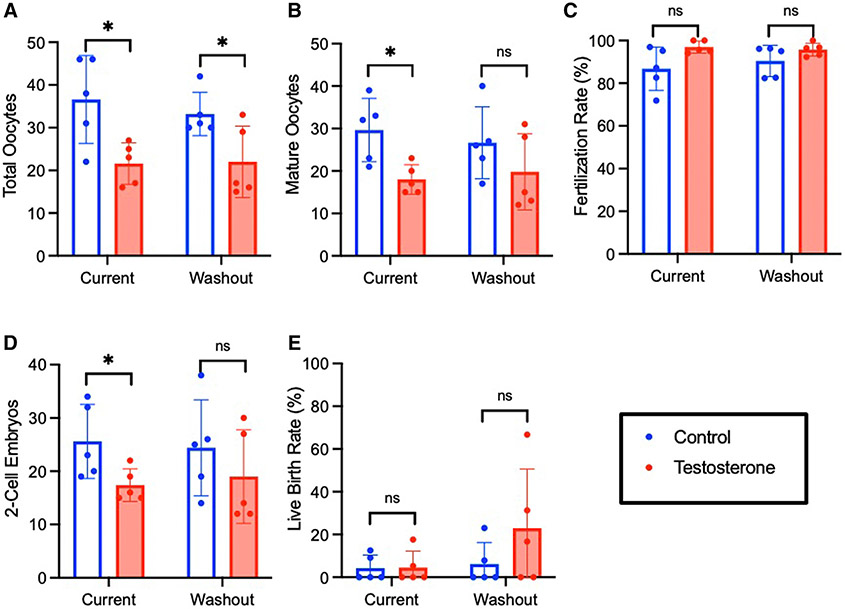
Results: Current long-term testosterone treatment impaired in vitro fertilization outcomes, with fewer mature oocytes retrieved (13.7±5.1 [standard deviation] vs 28.6±7.8 [standard deviation]; P<.0001) leading to fewer cleavage-stage embryos (12.1±5.1 vs 26.5±8.2; P<.0001) and blastocysts (10.0±3.2 vs 25.0±6.5; P<.0001). There was recovery of in vitro fertilization outcomes following washout in the short-term treatment cohort, with incomplete reversibility in the long-term cohort. Testosterone did not negatively affect maturity, fertilization, or blastulation rates.
Conclusion: In a mouse model of gender-affirming hormone treatment, testosterone negatively affected oocyte yield without affecting oocyte quality. Our findings suggest that testosterone reversibility is duration-dependent. These results demonstrate the feasibility of in vitro fertilization without testosterone discontinuation while supporting a washout period for optimization of mature oocyte yield.
Keywords: assisted reproductive technology; fertility; fertility preservation; transgender medicine.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Comment in
-
Patient au-T-onomy.Am J Obstet Gynecol. 2023 Oct;229(4):359-360. doi: 10.1016/j.ajog.2023.07.053. Epub 2023 Aug 21. Am J Obstet Gynecol. 2023. PMID: 37612218 No abstract available.
References
-
- Herman JL, Flores AR, O’Neill KK. How many adults and youth identify as transgender in the United States. The Williams Institute, UCLA School of Law; 2022.
-
- Winter S, Diamond M, Green J, et al. Transgender people: health at the margins of society. Lancet 2016;388:390–400. - PubMed
-
- Auer MK, Fuss J, Nieder TO, et al. Desire to have children among transgender people in Germany: a cross-sectional multi-center study. J Sex Med 2018;15:757–67. - PubMed
-
- Ethics Committee of the American Society for Reproductive Medicine. asrm@asrm.org. Access to fertility services by transgender and nonbinary persons: an Ethics Committee opinion. Fertil Steril 2021;115:874–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
