

Supra-additive effect of chronic inflammation and atherogenic dyslipidemia on developing type 2 diabetes among young adults: a prospective cohort study
- PMID: 37454077
- PMCID: PMC10350274
- DOI: 10.1186/s12933-023-01878-5
Supra-additive effect of chronic inflammation and atherogenic dyslipidemia on developing type 2 diabetes among young adults: a prospective cohort study
Abstract
Background: Both elevated inflammation and atherogenic dyslipidemia are prominent in young-onset diabetes and are increasingly identified as biologically intertwined processes that contribute to diabetogenesis. We aimed to investigate the age-specific risks of type 2 diabetes (T2D) upon concomitant chronic inflammation and atherogenic dyslipidemia.
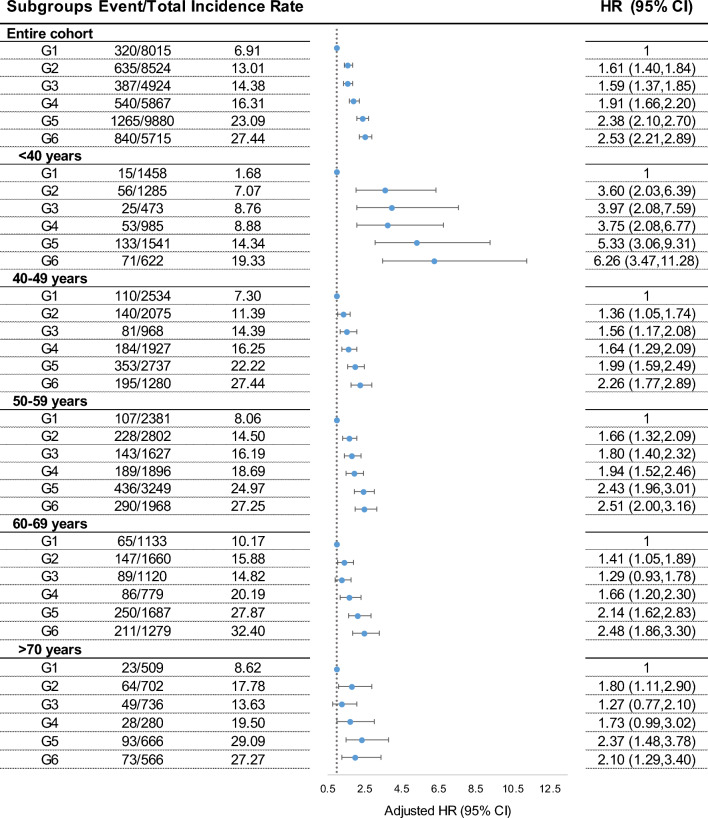
Methods: Age-stratified Cox regression analysis of the risk of incident diabetes upon co-exposure to time-averaged cumulative high-sensitivity C-reactive protein (CumCRP) and atherogenic index of plasma (CumAIP) among 42,925 nondiabetic participants from a real-world, prospective cohort (Kailuan Study).
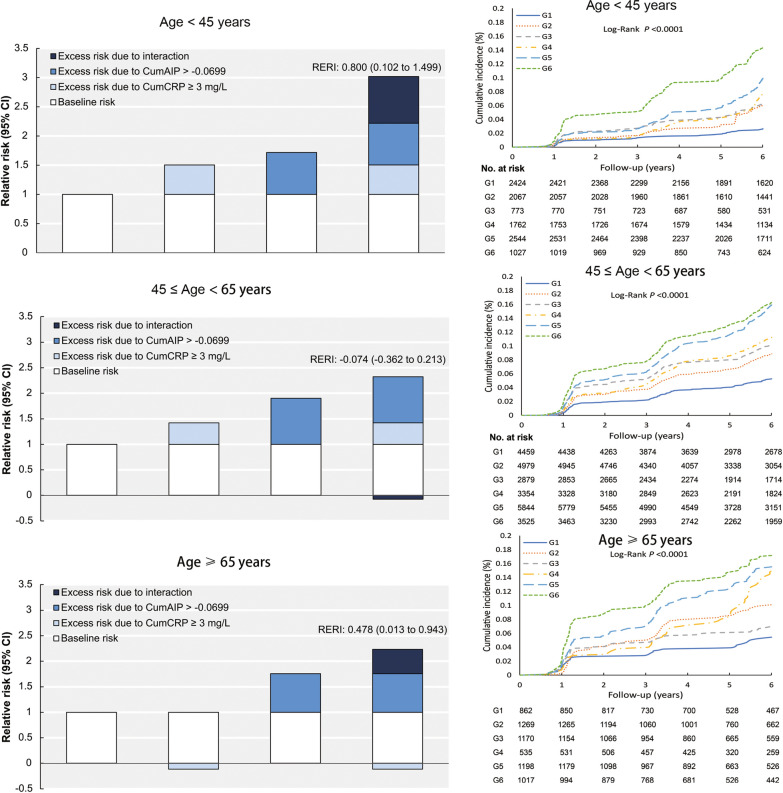
Results: During a median 6.41 years of follow-up, 3987 T2D developed. Isolated CumAIP and CumCRP were significantly associated with incident T2D in the entire cohort and across all age subgroups. Both CumAIP and CumCRP were jointly associated with an increased risk of diabetes (P-interaction = 0.0126). Compared to CumAIP < -0.0699 and CumCRP < 1 mg/L, co-exposure to CumAIP ≥ - 0.0699 and CumCRP ≥ 3 mg/L had a significant hazard ratio (HR) [2.55 (2.23-2.92)] after adjusting for socio-demographic, life-style factors, family history of diabetes, blood pressure, renal function and medication use. The co-exposure-associated risks varied greatly by age distribution (P-interaction = 0.0193): < 40 years, 6.26 (3.47-11.28); 40-49 years, 2.26 (1.77-2.89); 50-59 years, 2.51 (2.00-3.16); 60-69 years, 2.48 (1.86-3.30); ≥ 70 years, 2.10 (1.29-3.40). In young adults (< 45 years), both exposures had a significant supra-additive effect on diabetogenesis (relative excess risk due to interaction: 0.80, 95% CI 0.10-1.50).
Conclusions: These findings highlight the need for age-specific combined assessment and management of chronic inflammation and dyslipidemia in primary prevention against T2D, particularly for young adults. The clinical benefit derived from dual-target intervention against dyslipidemia and inflammation will exceed the sum of each part alone in young adults.
Keywords: Aging; Dyslipidemia; Inflammation; Type 2 diabetes; Young adults.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no potential competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
