

Differences in Mortality Among Patients With Asthma and COPD Hospitalized With COVID-19
- PMID: 37454926
- PMCID: PMC10787810
- DOI: 10.1016/j.jaip.2023.07.006
Differences in Mortality Among Patients With Asthma and COPD Hospitalized With COVID-19
Abstract
Background: It remains unclear whether patients with asthma and/or chronic obstructive pulmonary disease (COPD) are at increased risk for severe coronavirus disease 2019 (COVID-19).
Objective: Compare in-hospital COVID-19 outcomes among patients with asthma, COPD, and no airway disease.
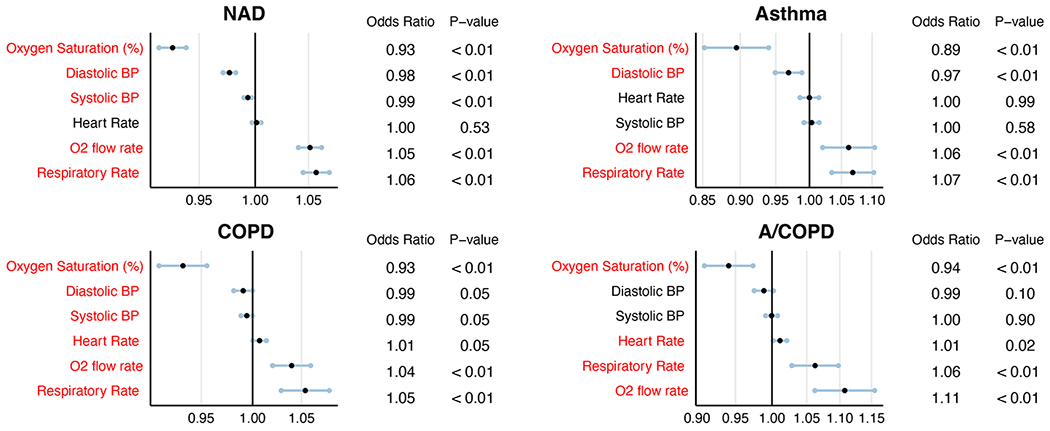
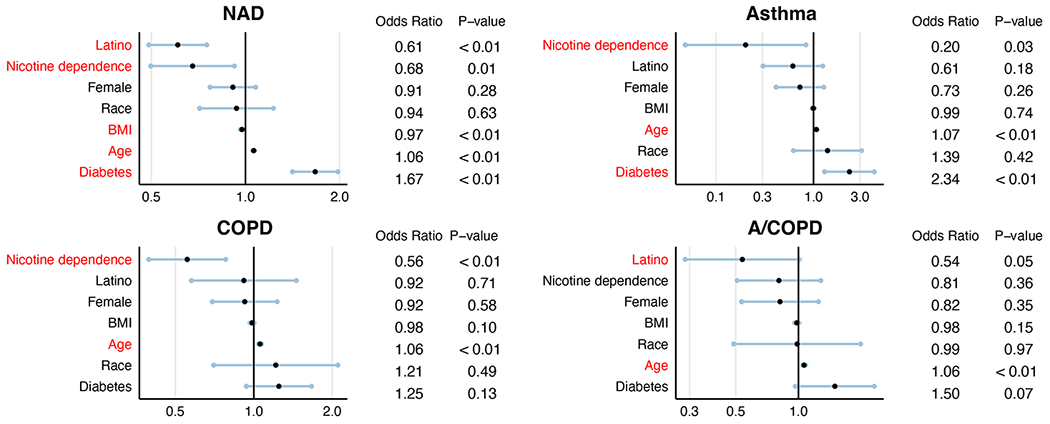
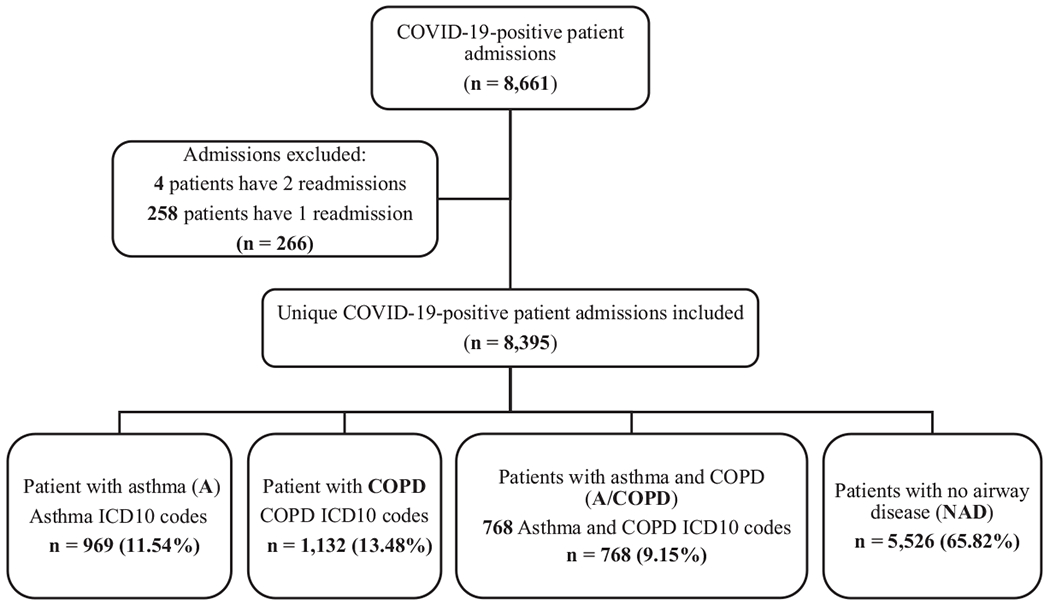
Methods: A retrospective cohort study was conducted on 8,395 patients admitted with COVID-19 between March 2020 and April 2021. Airway disease diagnoses were defined using International Classification of Diseases, 10th Revision codes. Mortality and sequential organ failure assessment (SOFA) scores were compared among groups. Logistic regression analysis was used to identify and adjust for confounding clinical features associated with mortality.
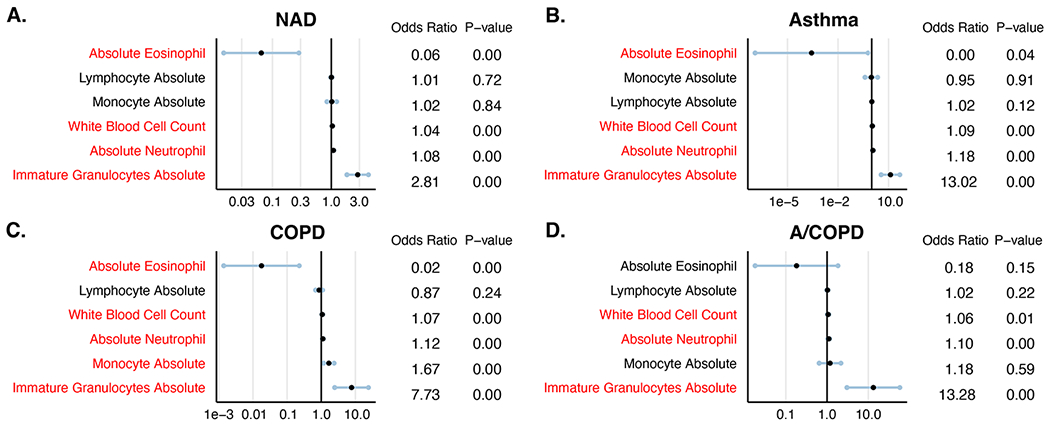
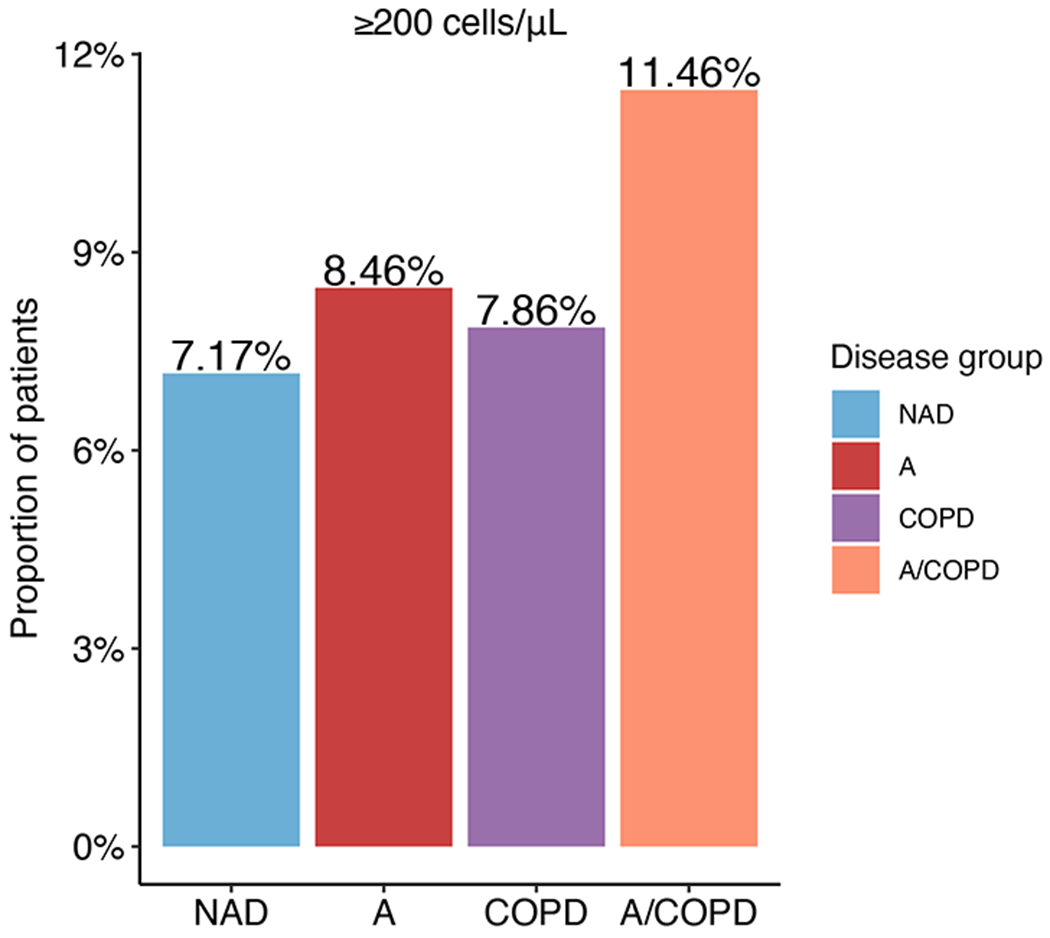
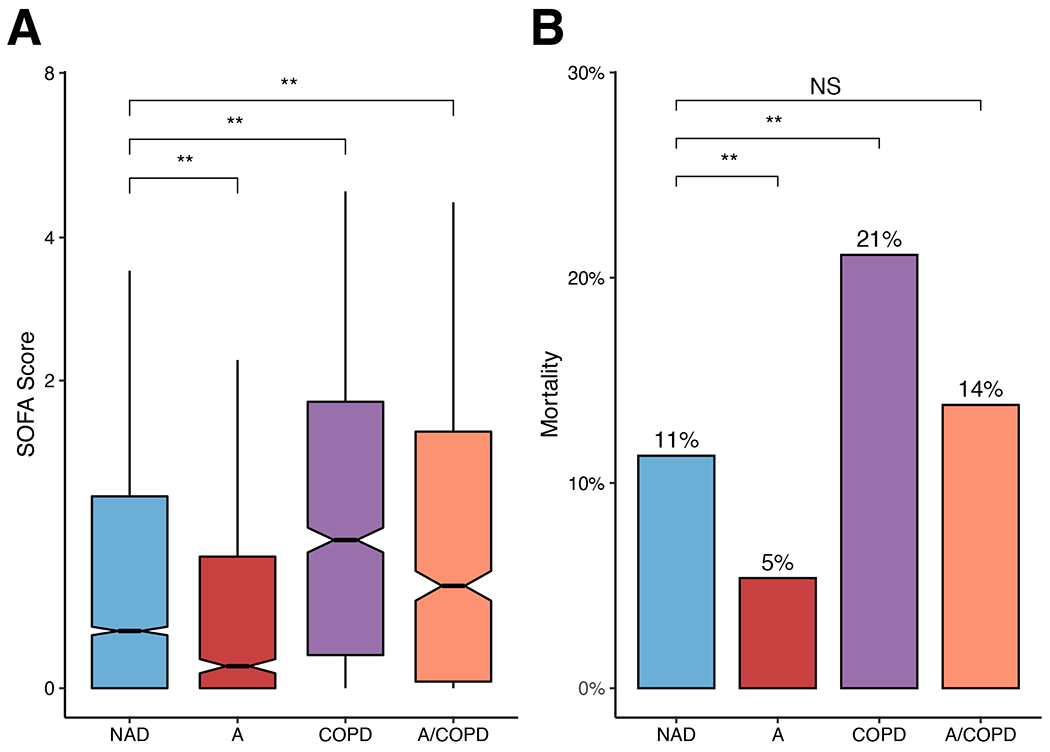
Results: The median SOFA score in patients without airway disease was 0.32 and mortality was 11%. In comparison, asthma patients had lower SOFA scores (median 0.15; P < .01) and decreased mortality, even after adjusting for age, diabetes, and other confounders (odds ratio 0.65; P = .01). Patients with COPD had higher SOFA scores (median 0.86; P < .01) and increased adjusted odds of mortality (odds ratio 1.40; P < .01). Blood eosinophil count of 200 cells/μL or greater, a marker of type 2 inflammation, was associated with lower mortality across all groups. Importantly, patients with asthma showed improved outcomes even after adjusting for eosinophilia, indicating that noneosinophilic asthma was associated with protection as well.
Conclusions: COVID-19 severity was increased in patients with COPD and decreased in those with asthma, eosinophilia, and noneosinophilic asthma, independent of clinical confounders. These findings suggest that COVID-19 severity may be influenced by intrinsic immunological factors in patients with airway diseases, such as type 2 inflammation.
Keywords: Asthma; COPD; COVID-19; Eosinophil; SARS-CoV-2.
Copyright © 2023 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- NCDC. Coronavirus disease (COVID-2019) situation reports. World Health Organisation; 2020;
-
- Wu Z, McGoogan JM. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA - Journal of the American Medical Association 2020;323:1239–1242. - PubMed
-
- Gao Y dong, Ding M, Dong X, Zhang J jin, Kursat Azkur A, Azkur D, et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy: European Journal of Allergy and Clinical Immunology 2021. ;76:428–455. - PubMed
-
- Centers of Diseases and Control Prevention. People with Certain Medical Conditions. Centers for Disease Control and Prevention; 2022;at <https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-...>.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
