

Metabolic dysfunction-associated gallstone disease: expecting more from critical care manifestations
- PMID: 37455265
- PMCID: PMC10543156
- DOI: 10.1007/s11739-023-03355-z
Metabolic dysfunction-associated gallstone disease: expecting more from critical care manifestations
Abstract
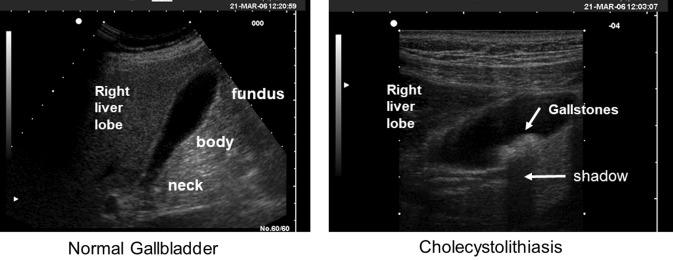
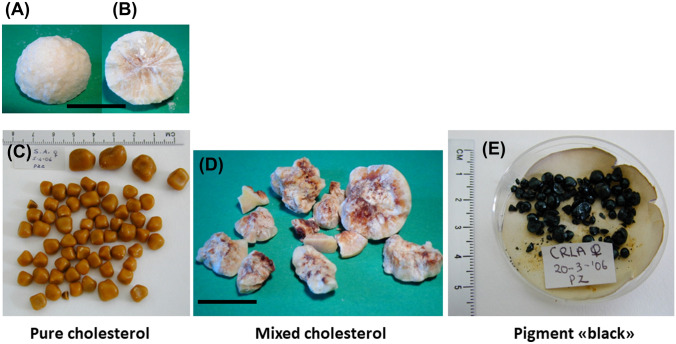
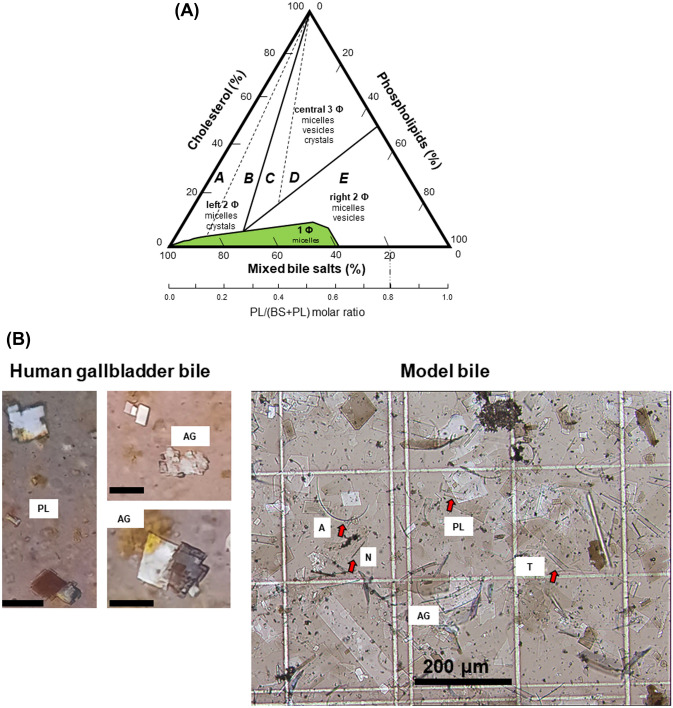
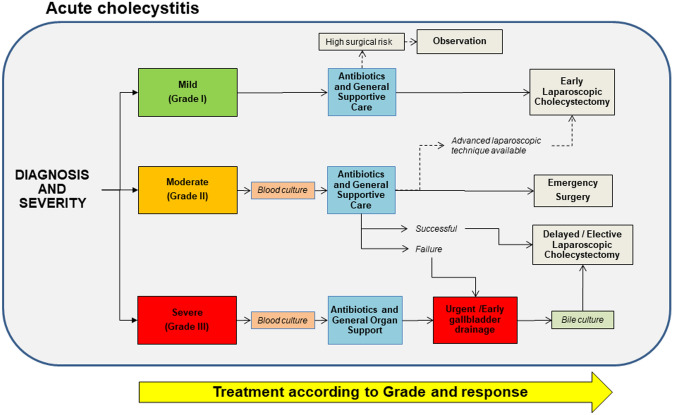
About 20% of adults worldwide have gallstones which are solid conglomerates in the biliary tree made of cholesterol monohydrate crystals, mucin, calcium bilirubinate, and protein aggregates. About 20% of gallstone patients will definitively develop gallstone disease, a condition which consists of gallstone-related symptoms and/or complications requiring medical therapy, endoscopic procedures, and/or cholecystectomy. Gallstones represent one of the most prevalent digestive disorders in Western countries and patients with gallstone disease are one of the largest categories admitted to European hospitals. About 80% of gallstones in Western countries are made of cholesterol due to disturbed cholesterol homeostasis which involves the liver, the gallbladder and the intestine on a genetic background. The incidence of cholesterol gallstones is dramatically increasing in parallel with the global epidemic of insulin resistance, type 2 diabetes, expansion of visceral adiposity, obesity, and metabolic syndrome. In this context, gallstones can be largely considered a metabolic dysfunction-associated gallstone disease, a condition prone to specific and systemic preventive measures. In this review we discuss the key pathogenic and clinical aspects of gallstones, as the main clinical consequences of metabolic dysfunction-associated disease.
Keywords: Bile; Biliary colic; Biliary secretion; CT scan; Cholecystectomy; Cholecystitis; Choledocholithiasis; Cholesterol crystallization; ERCP; MRCP.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Attili AF, Carulli N, Roda E, Barbara B, Capocaccia L, Menotti A, Okoliksanyi L, Ricci G, Capocaccia R, Festi D, et al. Epidemiology of gallstone disease in Italy: prevalence data of the Multicenter Italian Study on Cholelithiasis (M.I.COL.) Am J Epidemiol. 1995;141(2):158–165. doi: 10.1093/oxfordjournals.aje.a117403. - DOI - PubMed
-
- Farthing M, Roberts SE, Samuel DG, Williams JG, Thorne K, Morrison-Rees S, John A, Akbari A, Williams JC. Survey of digestive health across Europe: Final report. Part 1: The burden of gastrointestinal diseases and the organisation and delivery of gastroenterology services across Europe. United Eur Gastroenterol J. 2014;2(6):539–543. doi: 10.1177/2050640614554154. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
