

Serum proteome profiles in patients treated with targeted temperature management after out-of-hospital cardiac arrest
- PMID: 37455296
- PMCID: PMC10350448
- DOI: 10.1186/s40635-023-00528-0
Serum proteome profiles in patients treated with targeted temperature management after out-of-hospital cardiac arrest
Abstract
Background: Definition of temporal serum proteome profiles after out-of-hospital cardiac arrest may identify biological processes associated with severe hypoxia-ischaemia and reperfusion. It may further explore intervention effects for new mechanistic insights, identify candidate prognostic protein biomarkers and potential therapeutic targets. This pilot study aimed to investigate serum proteome profiles from unconscious patients admitted to hospital after out-of-hospital cardiac arrest according to temperature treatment and neurological outcome.
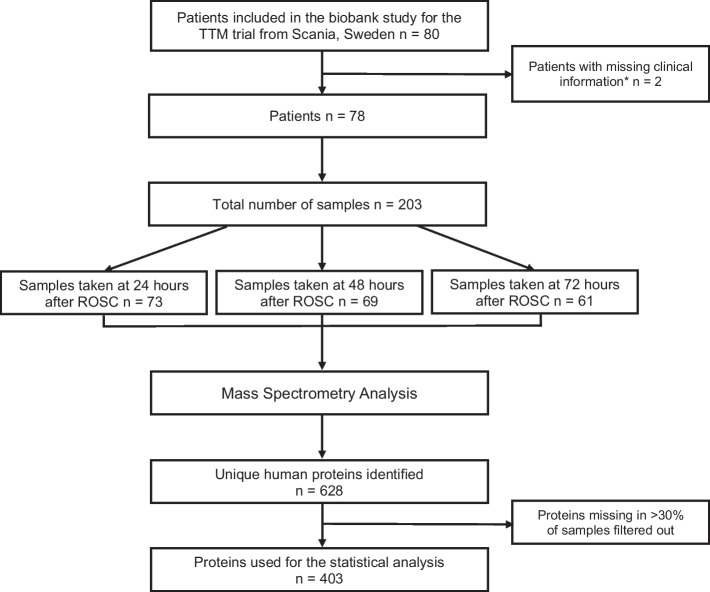
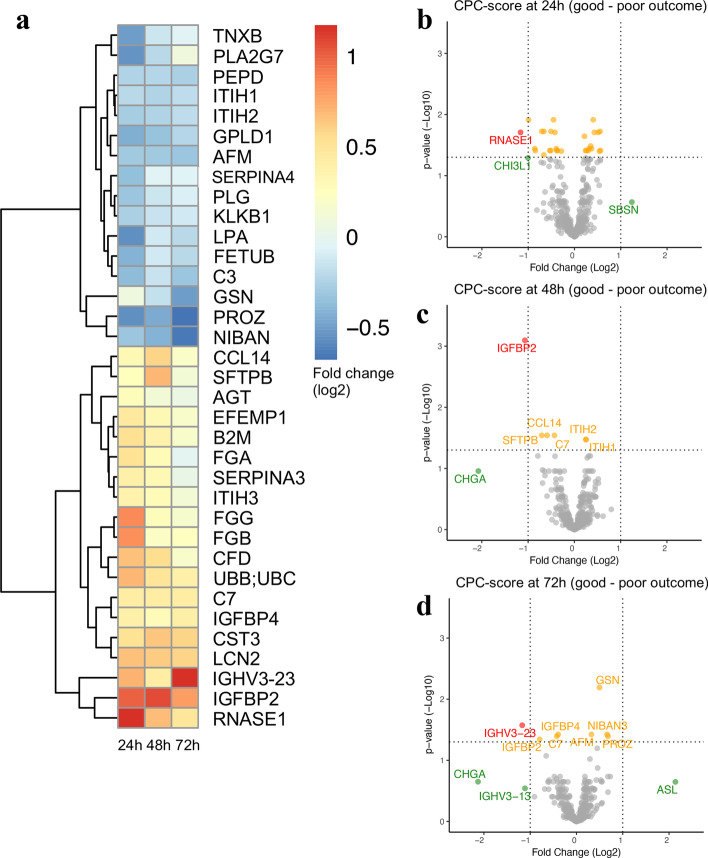
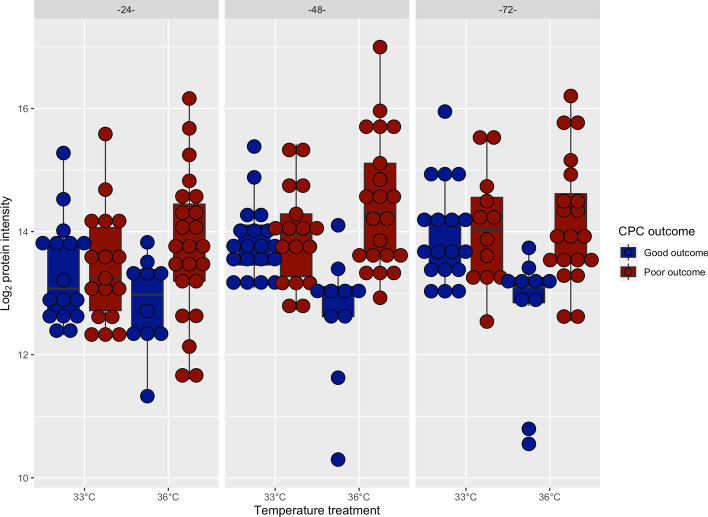
Methods: Serum samples at 24, 48, and 72 h after cardiac arrest at three centres included in the Target Temperature Management after out-of-hospital cardiac arrest trial underwent data-independent acquisition mass spectrometry analysis (DIA-MS) to find changes in serum protein concentrations associated with neurological outcome at 6-month follow-up and targeted temperature management (TTM) at 33 °C as compared to 36 °C. Neurological outcome was defined according to Cerebral Performance Category (CPC) scale as "good" (CPC 1-2, good cerebral performance or moderate disability) or "poor" (CPC 3-5, severe disability, unresponsive wakefulness syndrome, or death).
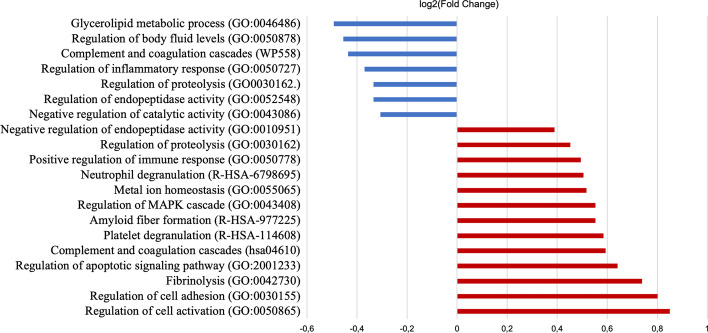
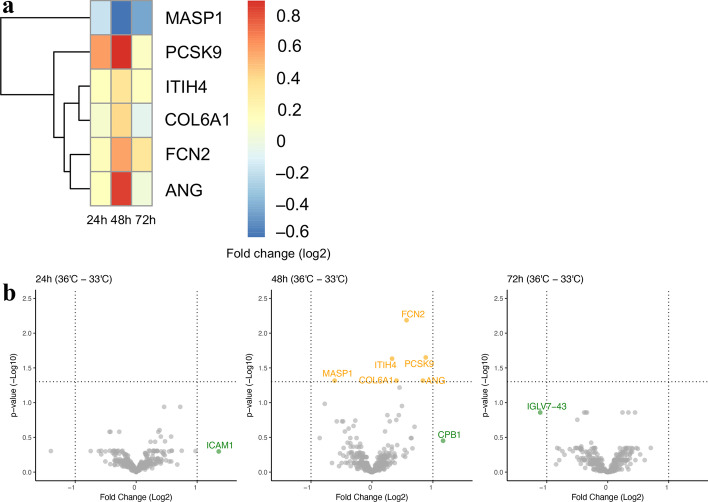
Results: Of 78 included patients [mean age 66 ± 12 years, 62 (80.0%) male], 37 (47.4%) were randomised to TTM at 36 °C. Six-month outcome was poor in 47 (60.3%) patients. The DIA-MS analysis identified and quantified 403 unique human proteins. Differential protein abundance testing comparing poor to good outcome showed 19 elevated proteins in patients with poor outcome (log2-fold change (FC) range 0.28-1.17) and 16 reduced proteins (log2(FC) between - 0.22 and - 0.68), involved in inflammatory/immune responses and apoptotic signalling pathways for poor outcome and proteolysis for good outcome. Analysis according to level of TTM showed a significant protein abundance difference for six proteins [five elevated proteins in TTM 36 °C (log2(FC) between 0.33 and 0.88), one reduced protein (log2(FC) - 0.6)] mainly involved in inflammatory/immune responses only at 48 h after cardiac arrest.
Conclusions: Serum proteome profiling revealed an increase in inflammatory/immune responses and apoptosis in patients with poor outcome. In patients with good outcome, an increase in proteolysis was observed, whereas TTM-level only had a modest effect on the proteome profiles. Further validation of the differentially abundant proteins in response to neurological outcome is necessary to validate novel biomarker candidates that may predict prognosis after cardiac arrest.
Keywords: Heart arrest; Hypothermia; Out-of-hospital cardiac arrest; Prognostication; Proteomics; Targeted temperature management; Temperature control.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, Böttiger BW, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication: a scientific statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation. 2008;79(3):350–379. doi: 10.1016/j.resuscitation.2008.09.017. - DOI - PubMed
-
- Geocadin RG, Callaway CW, Fink EL, Golan E, Greer DM, Ko NU, et al. Standards for studies of neurological prognostication in comatose survivors of cardiac arrest: a scientific statement from the American Heart Association. Circulation. 2019;140(9):e517–e542. doi: 10.1161/CIR.0000000000000702. - DOI - PubMed
-
- Adrie C, Adib-Conquy M, Laurent I, Monchi M, Vinsonneau C, Fitting C, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a "sepsis-like" syndrome. Circulation. 2002;106(5):562–568. doi: 10.1161/01.CIR.0000023891.80661.AD. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
