

MELD 3.0 adequately predicts mortality and renal replacement therapy requirements in patients with alcohol-associated hepatitis
- PMID: 37456675
- PMCID: PMC10339256
- DOI: 10.1016/j.jhepr.2023.100727
MELD 3.0 adequately predicts mortality and renal replacement therapy requirements in patients with alcohol-associated hepatitis
Abstract
Background & aims: Model for End-Stage Liver Disease (MELD) score better predicts mortality in alcohol-associated hepatitis (AH) but could underestimate severity in women and malnourished patients. Using a global cohort, we assessed the ability of the MELD 3.0 score to predict short-term mortality in AH.
Methods: This was a retrospective cohort study of patients admitted to hospital with AH from 2009 to 2019. The main outcome was all-cause 30-day mortality. We compared the AUC using DeLong's method and also performed a time-dependent AUC with competing risks analysis.
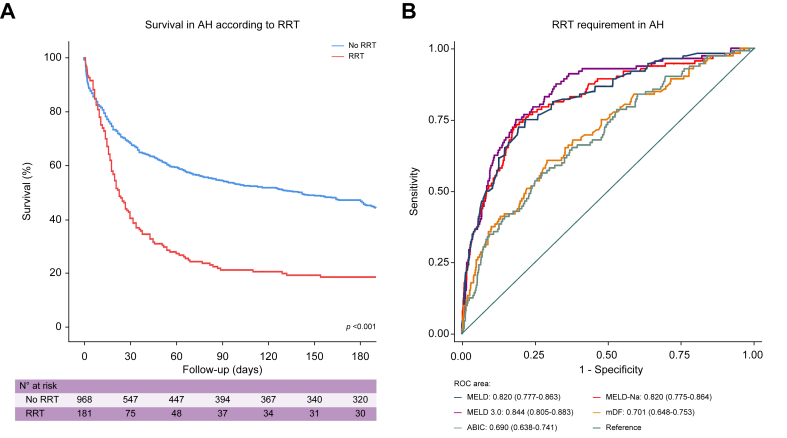
Results: A total of 2,124 patients were included from 28 centres from 10 countries on three continents (median age 47.2 ± 11.2 years, 29.9% women, 71.3% with underlying cirrhosis). The median MELD 3.0 score at admission was 25 (20-33), with an estimated survival of 73.7% at 30 days. The MELD 3.0 score had a better performance in predicting 30-day mortality (AUC:0.761, 95%CI:0.732-0.791) compared with MELD sodium (MELD-Na; AUC: 0.744, 95% CI: 0.713-0.775; p = 0.042) and Maddrey's discriminant function (mDF) (AUC: 0.724, 95% CI: 0.691-0.757; p = 0.013). However, MELD 3.0 did not perform better than traditional MELD (AUC: 0.753, 95% CI: 0.723-0.783; p = 0.300) and Age-Bilirubin-International Normalised Ratio-Creatinine (ABIC) (AUC:0.757, 95% CI: 0.727-0.788; p = 0.765). These results were consistent in competing-risk analysis, where MELD 3.0 (AUC: 0.757, 95% CI: 0.724-0.790) predicted better 30-day mortality compared with MELD-Na (AUC: 0.739, 95% CI: 0.708-0.770; p = 0.028) and mDF (AUC:0.717, 95% CI: 0.687-0.748; p = 0.042). The MELD 3.0 score was significantly better in predicting renal replacement therapy requirements during admission compared with the other scores (AUC: 0.844, 95% CI: 0.805-0.883).
Conclusions: MELD 3.0 demonstrated better performance compared with MELD-Na and mDF in predicting 30-day and 90-day mortality, and was the best predictor of renal replacement therapy requirements during admission for AH. However, further prospective studies are needed to validate its extensive use in AH.
Impact and implications: Severe AH has high short-term mortality. The establishment of treatments and liver transplantation depends on mortality prediction. We evaluated the performance of the new MELD 3.0 score to predict short-term mortality in AH in a large global cohort. MELD 3.0 performed better in predicting 30- and 90-day mortality compared with MELD-Na and mDF, but was similar to MELD and ABIC scores. MELD 3.0 was the best predictor of renal replacement therapy requirements. Thus, further prospective studies are needed to support the wide use of MELD 3.0 in AH.
Keywords: Alcohol; Alcoholic hepatitis; Cirrhosis; End-stage liver disease; Female; MELD; Outcome prediction.
© 2023 The Author(s).
Figures


References
-
- Díaz L.A., Idalsoaga F., Fuentes-López E., Márquez-Lomas A., Ramírez C.A., Roblero J.P., et al. Impact of public health policies on alcohol-associated liver disease in Latin America: an ecological multi-national study. Hepatology. 2021;74:2478–2490. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
