

Suicide prevention and ketamine: insights from computational modeling
- PMID: 37457775
- PMCID: PMC10342546
- DOI: 10.3389/fpsyt.2023.1214018
Suicide prevention and ketamine: insights from computational modeling
Abstract
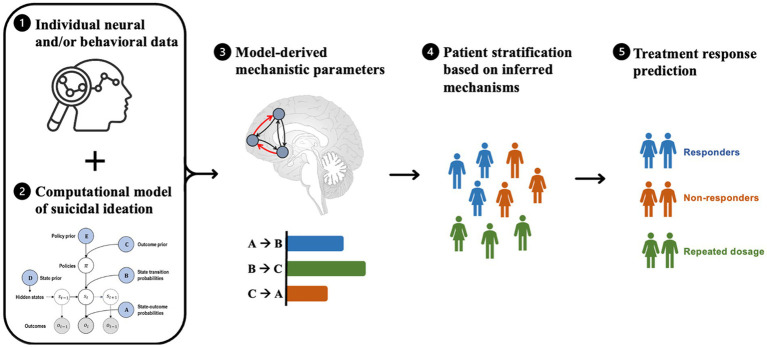
Suicide is a pressing public health issue, with over 700,000 individuals dying each year. Ketamine has emerged as a promising treatment for suicidal thoughts and behaviors (STBs), yet the complex mechanisms underlying ketamine's anti-suicidal effect are not fully understood. Computational psychiatry provides a promising framework for exploring the dynamic interactions underlying suicidality and ketamine's therapeutic action, offering insight into potential biomarkers, treatment targets, and the underlying mechanisms of both. This paper provides an overview of current computational theories of suicidality and ketamine's mechanism of action, and discusses various computational modeling approaches that attempt to explain ketamine's anti-suicidal effect. More specifically, the therapeutic potential of ketamine is explored in the context of the mismatch negativity and the predictive coding framework, by considering neurocircuits involved in learning and decision-making, and investigating altered connectivity strengths and receptor densities targeted by ketamine. Theory-driven computational models offer a promising approach to integrate existing knowledge of suicidality and ketamine, and for the extraction of model-derived mechanistic parameters that can be used to identify patient subgroups and personalized treatment approaches. Future computational studies on ketamine's mechanism of action should optimize task design and modeling approaches to ensure parameter reliability, and external factors such as set and setting, as well as psychedelic-assisted therapy should be evaluated for their additional therapeutic value.
Keywords: computational modeling; generative models; ketamine; psychiatry; suicidality.
Copyright © 2023 Charlton, Karvelis, McIntyre and Diaconescu.
Conflict of interest statement
RM has received research grant support from CIHR/GACD/National Natural Science Foundation of China (NSFC) and the Milken Institute; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, Abbvie, and Atai Life Sciences, and is a CEO of Braxia Scientific Corp. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- World Health Organisation Suicide (2021). Available at: https://www.who.int/news-room/fact-sheets/detail/suicide (Accessed June 16, 2022).
-
- Garnett MF, Curtin SC, Stone DM. Suicide mortality in the United States, 2000–2020. NCHS data brief, no 433. Hyattsville, MD: National Center for Health Statistics (2022). - PubMed
Publication types
LinkOut - more resources
Full Text Sources