

Risk of recurrent stroke in patients with atrial fibrillation treated with oral anticoagulants alone or in combination with anti-platelet therapy
- PMID: 37458099
- PMCID: PMC10472945
- DOI: 10.1177/23969873231183211
Risk of recurrent stroke in patients with atrial fibrillation treated with oral anticoagulants alone or in combination with anti-platelet therapy
Abstract
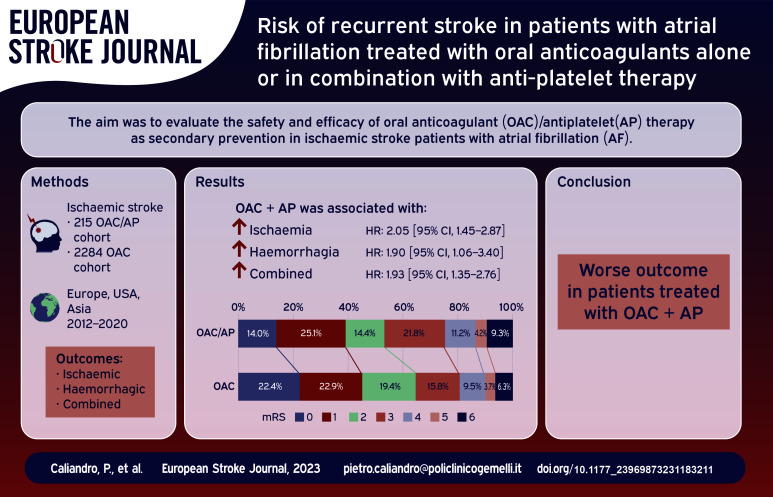
Introduction: Ischaemic stroke patients with atrial fibrillation (AF) are at high risk of stroke recurrence despite oral anticoagulation therapy. Patients with cardiovascular comorbidities may take both antiplatelet and oral anticoagulation therapy (OAC/AP). Our study aims to evaluate the safety and efficacy of OAC/AP therapy as secondary prevention in people with AF and ischaemic stroke.
Patients and methods: We performed a post-hoc analysis of pooled individual data from multicenter prospective cohort studies and compared outcomes in the OAC/AP cohort and patients on DOAC/VKA anticoagulation alone (OAC cohort). Primary outcome was a composite of ischaemic stroke, systemic embolism, intracranial bleeding, and major extracranial bleeding, while secondary outcomes were ischaemic and haemorrhagic events considered separately. A multivariable logistic regression analysis was performed to identify independent predictors for outcome events. To compare the risk of outcome events between the two cohorts, the relation between the survival function and the set of explanatory variables were calculated by Cox proportional hazard models and the results were reported as adjusted hazard ratios (HR). Finally another analysis was performed to compare the overall risk of outcome events in both OAC/AP and OAC cohorts after propensity score matching (PSM).
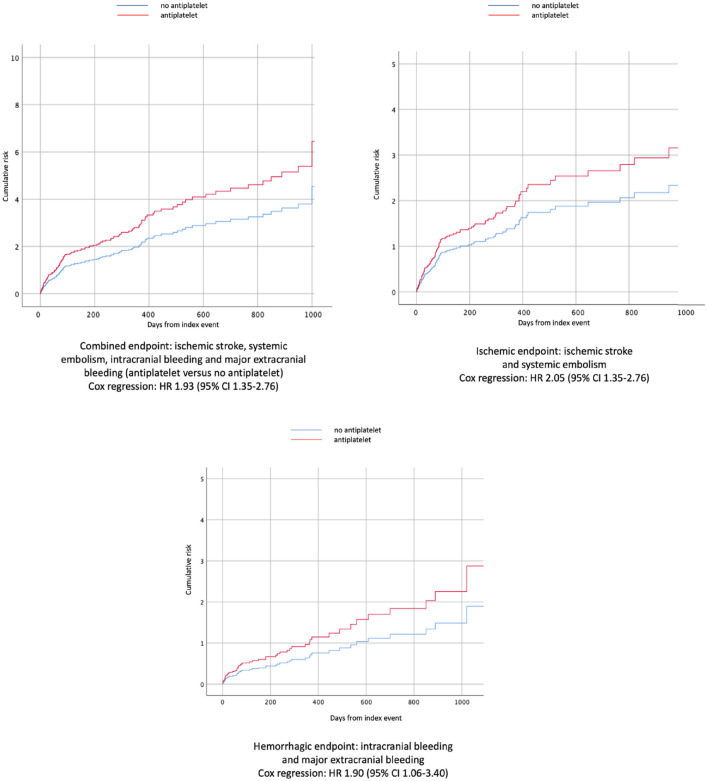
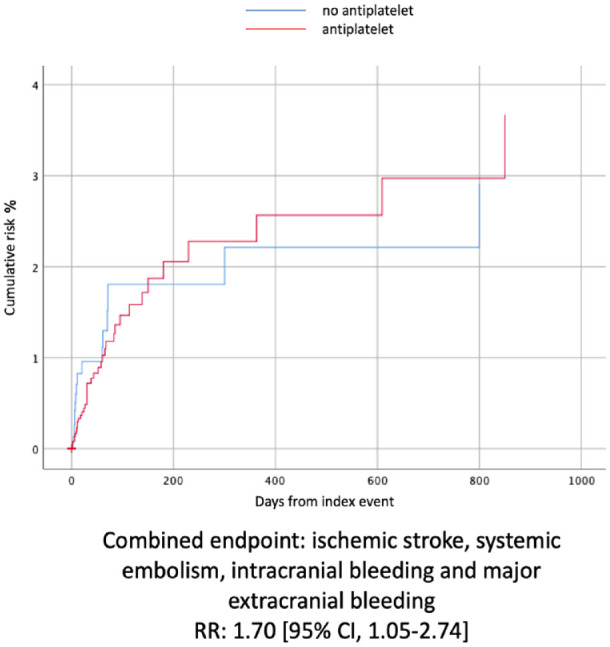
Results: During a mean follow-up time of 7.5 ± 9.1 months (median follow-up time 3.5 months, interquartile range ±3), 2284 stroke patients were on oral anticoagulants and 215 were on combined therapy. The multivariable model demonstrated that the composite outcome is associated with age (OR: 1.03, 95% CI: 1.01-1.04 for each year increase) and concomitant antiplatelet therapy (OR: 2.2, 95% CI: 1.48-3.27), the ischaemic outcome with congestive heart failure (OR: 1.55, 95% CI: 1.02-2.36) and concomitant antiplatelet therapy (OR: 1.93, 95% CI: 1.19-3.13) and the haemorrhagic outcome with age (OR: 1.03, 95% CI: 1.01-1.06 for each year increase), alcoholism (OR: 2.15, 95% CI: 1.06-4.39) and concomitant antiplatelet therapy (OR: 2.22, 95% CI: 1.23-4.02). Cox regression demonstrated a higher rate of the composite outcome (hazard ratio of 1.93 [95% CI, 1.35-2.76]), ischaemic events (HR: 2.05 [95% CI: 1.45-2.87]) and bleeding outcomes (HR: 1.90 [95% CI, 1.06-3.40]) in OAC/AP cohort. After PSM analysis, the composite outcome remained more frequent in people treated with OAC + AP (RR: 1.70 [95% CI, 1.05-2.74]).
Discussion: Secondary prevention with combination of oral anticoagulant and antiplatelet therapy after ischaemic stroke was associated with worse outcomes in our cohort.
Conclusion: Further research is needed to improve secondary prevention by investigating the mechanisms of recurrent ischaemic stroke in patients with atrial fibrillation.
Keywords: Ischaemic stroke; anticoagulants; antiplatelet; atrial fibrillation; secondary prevention.
Conflict of interest statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Diener H-C, Connolly SJ, Ezekowitz MD, et al. Dabigatran compared with warfarin in patients with atrial fibrillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE-LY trial. Lancet Neurol 2010; 9: 1157–1163. - PubMed
-
- Hankey GJ, Patel MR, Stevens SR, et al. Rivaroxaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of ROCKET AF. Lancet Neurol 2012; 11: 315–322. - PubMed
-
- Easton JD, Lopes RD, Bahit MC, et al. Apixaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of the ARISTOTLE trial. Lancet Neurol 2012; 11: 503–511. - PubMed
-
- Rost NS, Giugliano RP, Ruff CT, et al. Outcomes with edoxaban versus warfarin in patients with previous cerebrovascular events: findings from ENGAGE AF-TIMI 48 (Effective anticoagulation with factor Xa next generation in atrial fibrillation-thrombolysis in myocardial infarction 48). Stroke 2016; 47: 2075–2082. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
