

Real world data in mechanical thrombectomy: who are we losing to follow-up?
- PMID: 37460214
- PMCID: PMC11041564
- DOI: 10.1136/jnis-2023-020435
Real world data in mechanical thrombectomy: who are we losing to follow-up?
Abstract
Background: Missing outcome data (MOD) is a common problem in clinical trials and registries, and a potential bias when drawing conclusions from these data. Identifying factors associated with MOD may help to increase follow-up rates and assess the need for imputation strategies. We investigated MOD in a multicenter, prospective registry study of mechanical thrombectomy (MT) in large vessel occlusion ischemic stroke.
Methods: 13 082 patients enrolled in the German Stroke Registry-Endovascular Treatment from May 2015 to December 2021 were analyzed with regard to MOD (90 day modified Rankin Scale, mRS). Univariate logistic regression analyses identified factors unbalanced between patients with and without MOD. Subgroup analyses were performed to identify patients for whom increased efforts to perform clinical follow-up after hospital discharge are needed.
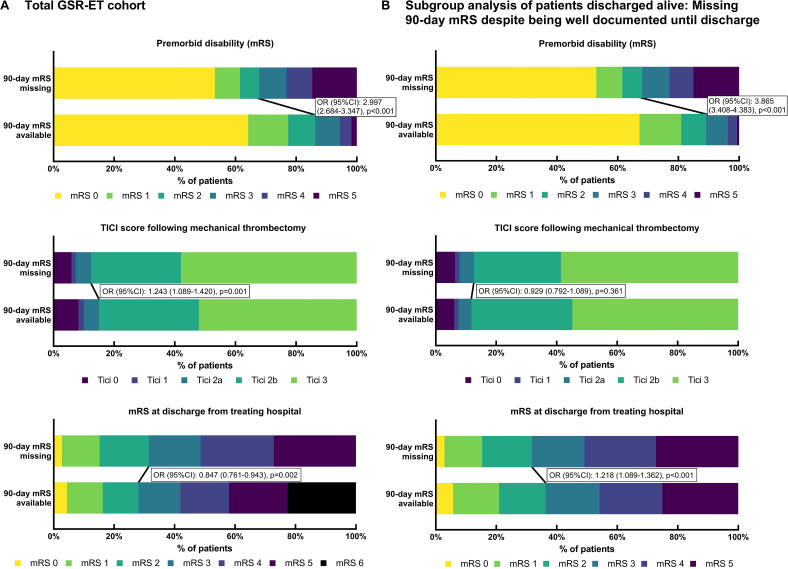
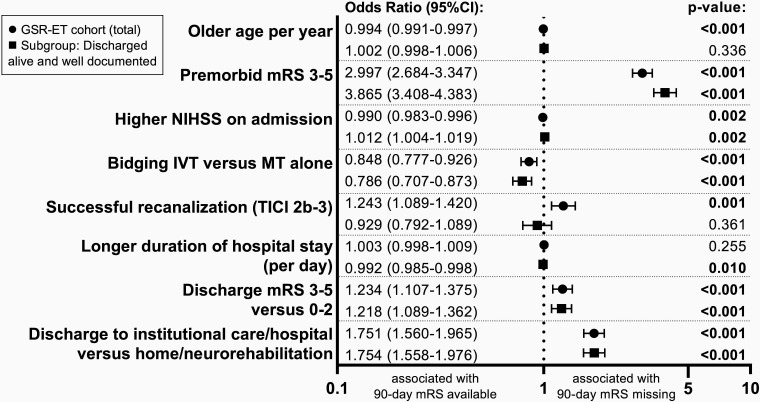
Results: We identified 19.7% (2580/13 082) of patients with MOD at the 90 day follow-up. MOD was more common with higher pre-stroke disability (mRS 3-5, 32.2% vs mRS 0-2, 13.7%; P<0.001), absence of bridging intravenous thrombolysis, longer time to treatment, and in patients with high post-stroke disability at discharge (mRS 3-5 vs 0-2: OR 1.234 (95% CI 1.107 to 1.375); P<0.001). In contrast, MOD was less common with futile recanalization (thrombolysis in cerebral infarction (TICI) score of 0-2a, 12.4% vs TICI 2b-3, 15.0%; P=0.001). In patients discharged alive with well documented baseline characteristics, shorter hospital stay (OR 0.992 (95% CI 0.985 to 0.998); P=0.010) and discharge to institutional care or hospital (OR 1.754 (95% CI 1.558 to 1.976); P<0.001) were associated with MOD.
Conclusion: MOD in routine care MT registry data was not random. Increased efforts to perform clinical follow-up are needed, especially in the case of higher pre-stroke and post-stroke disability and discharge to hospital or institutional care.
Trial registration: NCT03356392.
Keywords: Stroke; Thrombectomy.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AO reports speakers bureau from Cerenovus and Canon Medical. KG reports personal fees and/or non-financial support from Bayer, Boehringer Ingelheim, Bristol-Meyers Squibb, Daiichi Sankyo, and Pfizer. MH reports personal fees from Bristol-Meyers Squibb, outside of the submitted work. TU reports personal fees from Merck Serono and Pfizer, and grants from Else Kröner-Fresenius Stiftung.
Figures
Similar articles
-
Predictors of futile recanalization in ischemic stroke patients with low baseline NIHSS.Int J Stroke. 2024 Dec;19(10):1102-1112. doi: 10.1177/17474930241264737. Epub 2024 Nov 19. Int J Stroke. 2024. PMID: 38888031 Free PMC article.
-
Sex-Related Differences in Outcomes of Endovascular Treatment in Large Vessel Occlusion Stroke-Analyses From the German Stroke Registry-Endovascular Treatment.Eur J Neurol. 2025 Mar;32(3):e70092. doi: 10.1111/ene.70092. Eur J Neurol. 2025. PMID: 40008680 Free PMC article.
-
Comparison of Thrombolysis In Cerebral Infarction (TICI) 2b and TICI 3 reperfusion in endovascular therapy for large ischemic anterior circulation strokes.J Neurointerv Surg. 2024 Oct 14;16(11):1076-1082. doi: 10.1136/jnis-2023-020724. J Neurointerv Surg. 2024. PMID: 37777256 Free PMC article.
-
Endovascular thrombectomy for childhood stroke (Save ChildS Pro): an international, multicentre, prospective registry study.Lancet Child Adolesc Health. 2024 Dec;8(12):882-890. doi: 10.1016/S2352-4642(24)00233-5. Epub 2024 Oct 11. Lancet Child Adolesc Health. 2024. PMID: 39401507 Clinical Trial.
-
Feasibility and safety of thrombectomy for isolated occlusions of the posterior cerebral artery: a multicenter experience and systematic literature review.J Neurointerv Surg. 2021 Mar;13(3):217-220. doi: 10.1136/neurintsurg-2020-016059. Epub 2020 Jun 11. J Neurointerv Surg. 2021. PMID: 32527938
Cited by
-
[Focus neurological intensive care medicine 2023/2024 : Summary of selected studies in intensive medical care].Anaesthesiologie. 2025 Jan;74(1):38-49. doi: 10.1007/s00101-024-01490-6. Epub 2024 Dec 4. Anaesthesiologie. 2025. PMID: 39633141 German. No abstract available.
-
Sex Disparities in the Direct Cost and Management of Stroke: A Population-Based Retrospective Study.Healthcare (Basel). 2024 Jul 9;12(14):1369. doi: 10.3390/healthcare12141369. Healthcare (Basel). 2024. PMID: 39057512 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical