

Distributional impact of infectious disease interventions in the Ethiopian Essential Health Service Package: a modelling study
- PMID: 37460265
- PMCID: PMC10357664
- DOI: 10.1136/bmjopen-2022-067658
Distributional impact of infectious disease interventions in the Ethiopian Essential Health Service Package: a modelling study
Abstract
Objectives: Reducing inequalities in health and financial risk are key goals on the path toward universal health coverage, particularly in low-income and middle-income countries. The design of the health benefit package creates an opportunity to select interventions through established criteria. The aim of this study is to examine the health equity and financial protection impact of selected interventions, along with their costs, at the national level in Ethiopia.
Design: Distributional cost-effectiveness analysis.
Population: The eligible population for all selected interventions is assumed to be 10 million.
Data sources: Data on disease prevalence and population size were gathered from the Global Burden of Disease database, and average health benefits and program costs are sourced from the Ethiopian Essential Health Service Package (EHSP) database, national surveys and other publicly available sources.
Intervention: A total of 30 interventions were selected from the latest EHSP revision and analysed over a 1-year period.
Outcome measures: Health benefits, social welfare indices and financial protection metrics across income quintiles were reported.
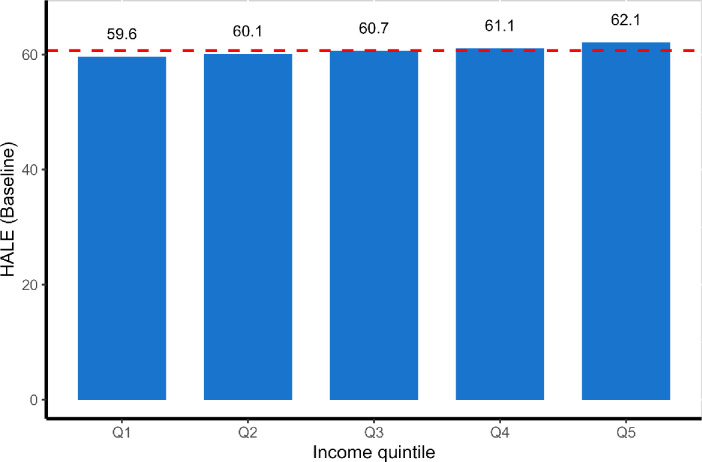
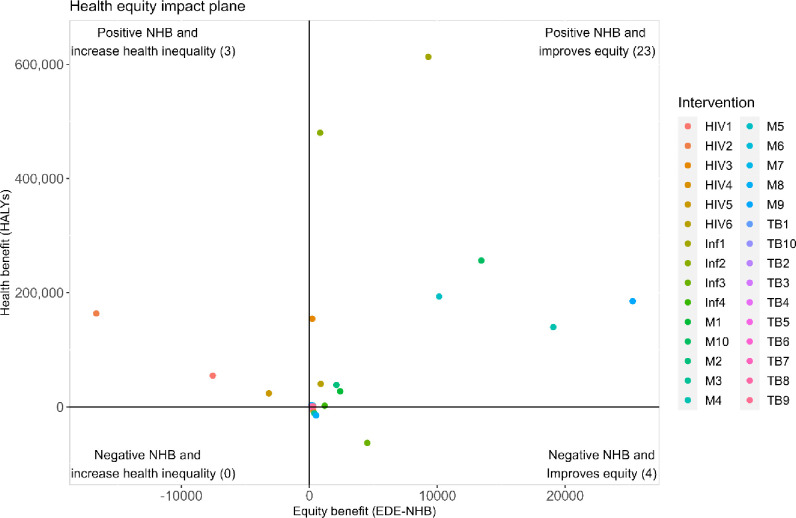
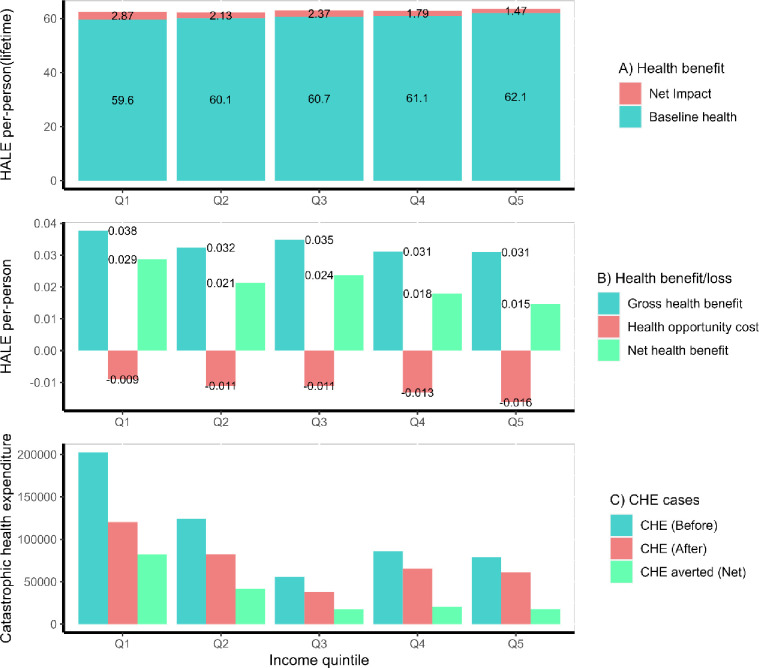
Results: We found 23 interventions that improve population health and reduce health inequality and four interventions reduce both population health and health inequality. Additionally, three interventions improve population health while increasing health inequality. Overall, the EHSP interventions provide a 0.021 improvement in health-adjusted life expectancy (HALE) per person, with a positive distributional equity impact: 0.029 (26.9%) HALE gained in the poorest and 0.015 (14.0%) in the richest quintile. Similarly, a total of 1 79 475 cases of catastrophic health expenditure were averted, including 82 100 (46.0%) cases in the poorest and 17 900 (10.0%) in the richest quintile.
Conclusion: Increasing access to the EHSP improves health equity and financial protection. Improved access to selected EHSP interventions also has the potential to provide greater benefits to the poorest and thereby improve social welfare.
Keywords: Ethiopia; distributional analysis; economic evaluation; financial risk protection; health inequality.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Roberts MJ, Hsiao W, Berman P, et al. . Getting health reform right, anniversary edition: a guide to improving performance and equity. New York: Oxford University Press, Incorporated, 2019.
-
- Eyal N, Hurst SA, Norheim OF, et al. . Inequalities in health. In: Fair society, healthy lives. Firenze: Leo S. Olschki, 2013. 10.1093/acprof:oso/9780199931392.001.0001 - DOI
-
- Sheiham A. Closing the gap in a generation: health equity through action on the social determinants of health. A report of the WHO commission on social determinants of health (CSDH) 2008. Community Dent Health 2009;26:2–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical