

Cardiovascular and renal multimorbidity increase risk of atrial fibrillation in the PREVEND cohort
- PMID: 37460268
- PMCID: PMC10357795
- DOI: 10.1136/openhrt-2023-002315
Cardiovascular and renal multimorbidity increase risk of atrial fibrillation in the PREVEND cohort
Abstract
Objective: Atrial fibrillation (AF) is a condition that occurs in the presence of comorbidities. With the accumulation of comorbidities (multimorbidity), some combinations may more often occur together than others. Information on the impact of clustering of these on incident AF is sparse. We aimed to investigate clustering of cardiovascular and renal comorbidities and study the association between comorbidity clusters and incident AF.
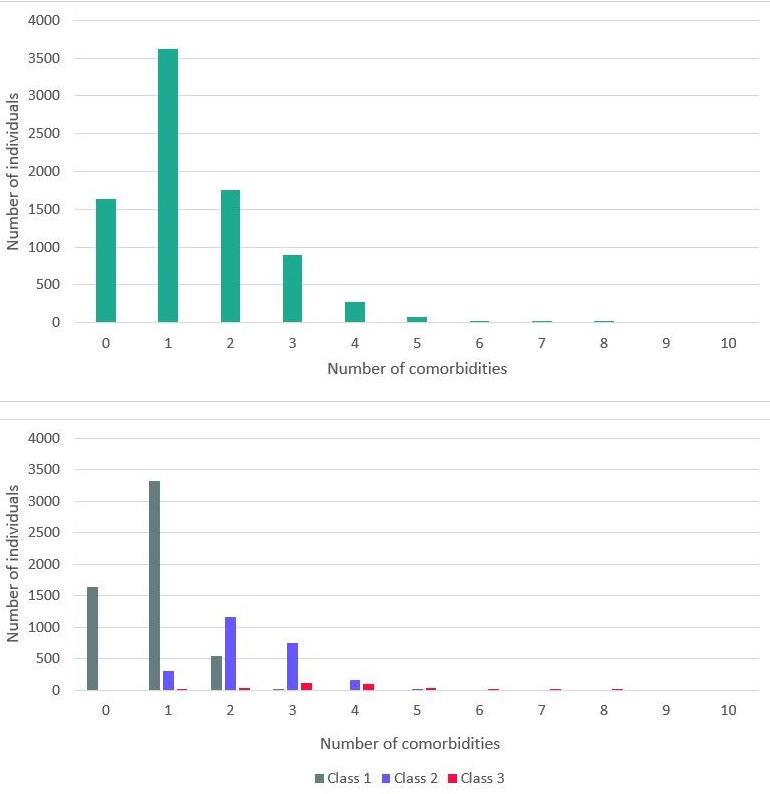
Methods: We used the community-based Prevention of Renal and Vascular ENd-stage Disease (PREVEND) cohort in which 8592 individuals participated. Latent class analysis was performed to assess clustering of 10 cardiovascular and renal comorbidities.
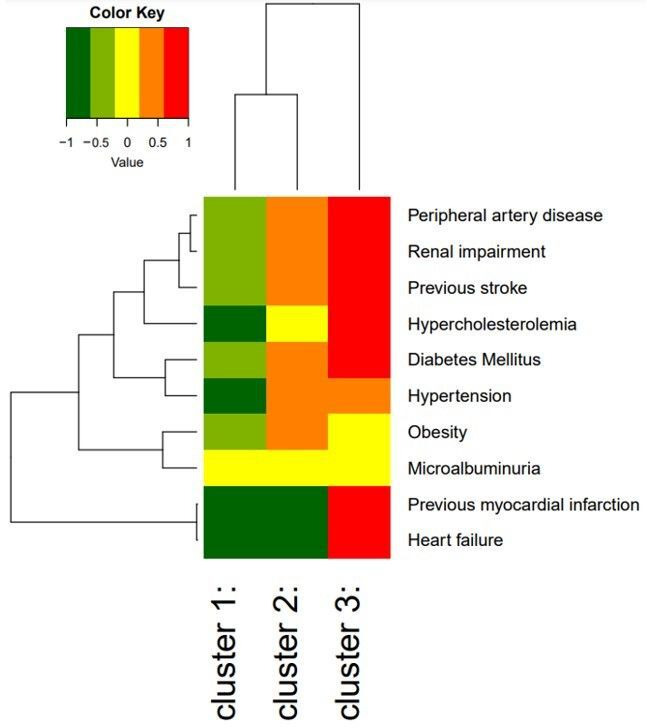
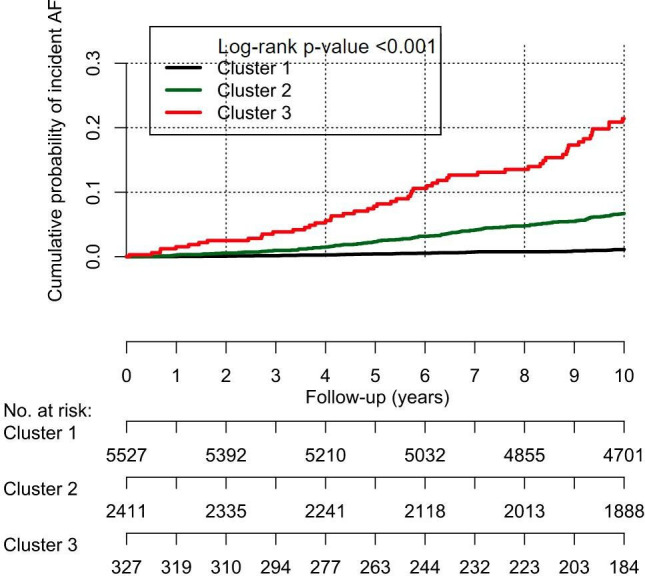
Results: We excluded individuals with prior AF or missing ECG data, leaving 8265 individuals for analysis (mean age 48.9±12.6 years, 50.2% women). During 9.2±2.1 years of follow-up, 251 individuals (3.0%) developed AF. A model with three clusters was the optimal model, with one cluster being young (44.5±10.8 years) and healthy, carrying a low (1.0%) risk of incident AF; one cluster being older (63.0±8.4 years) and multimorbid, carrying a high (16.2%) risk of incident AF and a third middle-aged (57.0±11.3 years), obese and hypertensive cluster carrying an intermediate risk (5.9%) of incident AF. While the prevalence of the comorbidities differed between classes, no clear combination(s) of comorbidities was observed within the classes.
Conclusions: We identified three clusters of comorbidities in individuals in the community-based PREVEND cohort. The three clusters contained different amount of comorbidities carrying different risks of incident AF. However, there were no differences between the clusters regarding specific combination(s) of comorbidities.
Keywords: Atrial Fibrillation; EPIDEMIOLOGY; RISK FACTORS.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: For the current manuscript, the authors declare no potential conflicts of interest. Outside of the submitted work, the authors disclosed the following financial support: MR reports grants from the Dutch Heart Foundation (CVON RACE V, grant 2014-09; CVON RED-CVD, grant 2017-11; CVON-AI, grant 2018B017; DECISION, grant 2018B024). The UMCG, which employs MR, has received grants from SJM/Abbott (VIP-HF study) and Medtronic (Cryoballoon AF registry/biobank study). ICVG reports grants from the Dutch Heart Foundation (CVON RACE V, grant 2014-09).
Figures
References
-
- Benjamin EJ, Levy D, Vaziri SM, et al. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham heart study. JAMA 1994;271:840–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical