

A novel technique of penetrating keratoplasty to prevent intraocular contents extrusion for infectious keratitis
- PMID: 37460970
- PMCID: PMC10351116
- DOI: 10.1186/s12886-023-03025-w
A novel technique of penetrating keratoplasty to prevent intraocular contents extrusion for infectious keratitis
Abstract
Purpose: To evaluate the safety and the effectiveness of our novel penetrating keratoplasty for infectious keratitis.
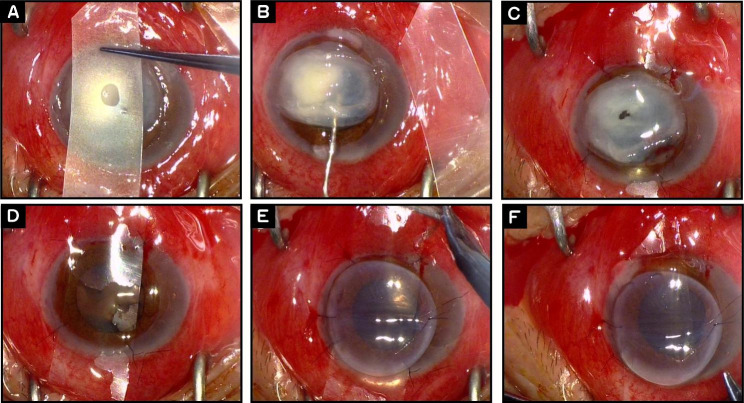
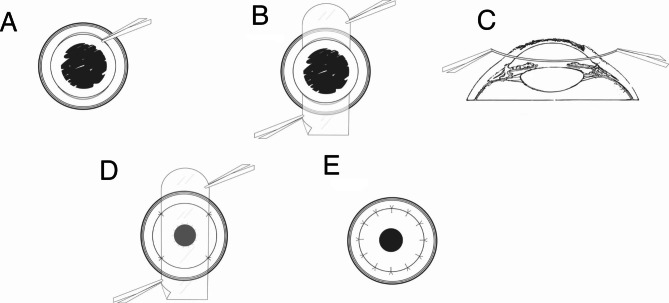
Methods: Retrospective, noncomparative, interventional case series of patients with infectious keratitis who received the novel penetrating keratoplasty technique were analyzed. A prepared plastic sheet was located between the diseased cornea and iris-lens diaphragm. After the diseased lesions were removed, the graft was positioned on the plastic sheet and sutured to the recipient bed. The plastic sheet was pulled out from the anterior chamber before the all interrupted sutures were placed. The intra- and post-operative complications, the outcome of the graft and the number of corneal endothelial cells were analyzed.
Results: A total of 82 eyes of 82 patients was included. The mean follow-up period was 29 ± 16 months (range from 13 to 45 months). No intraocular content extrusion, simultaneous cataract extraction and suprachoroidal hemorrhage occurred. Direct contact between the infectious cornea and the graft was successfully avoided. Greater than expected endothelial cell reduction or complications were not found.
Conclusions: This modified technique effectively prevents the extrusion of intraocular contents while avoiding the direct contact with donor endothelium during the procedure. The occurrence rate of complications such as endothelial cell loss is not higher than the conventional methods.
Keywords: Extrusion; Infectious keratitis; Intraocular contents; Lens-iris diaphragm; Penetrating keratoplasty; Plastic sheet.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Method for safer penetrating keratoplasty in patients with low scleral rigidity.J Cataract Refract Surg. 1999 Jul;25(7):882-4. doi: 10.1016/s0886-3350(99)00071-1. J Cataract Refract Surg. 1999. PMID: 10404360 Clinical Trial.
-
Iris-sutured posterior chamber intraocular lens implantation during penetrating keratoplasty.Cornea. 2004 Jan;23(1):18-28. doi: 10.1097/00003226-200401000-00004. Cornea. 2004. PMID: 14701953
-
Prognostic Factors Affecting Graft Survival in Patients Undergoing Penetrating Keratoplasty for Infectious Keratitis.Turk J Ophthalmol. 2020 Dec 29;50(6):324-331. doi: 10.4274/tjo.galenos.2020.35305. Turk J Ophthalmol. 2020. PMID: 33389931 Free PMC article.
-
Nonmechanical excimer laser penetrating keratoplasty for perforated or predescemetal corneal ulcers.Ophthalmology. 1999 Nov;106(11):2203-9. doi: 10.1016/S0161-6420(99)90506-7. Ophthalmology. 1999. PMID: 10571360
-
Therapeutic penetrating keratoplasty in severe fungal keratitis using cryopreserved donor corneas.Br J Ophthalmol. 2003 May;87(5):543-7. doi: 10.1136/bjo.87.5.543. Br J Ophthalmol. 2003. PMID: 12714387 Free PMC article.
References
-
- Price FW, Jr, Whitson WE, Ahad KA, et al. Suprachoroidal hemorrhage in penetrating keratoplasty. Ophthalmic Surg. 1994;25(8):521–54. - PubMed
-
- Lopez-Plandolit S, Etxebarria J, Acera A, et al. Protected penetrating keratoplasty: surgical technique and endothelial response. Arch Soc Esp Oftalmol. 2008;83(4):231–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
