

Unraveling the epigenetic landscape of pulmonary arterial hypertension: implications for personalized medicine development
- PMID: 37461108
- PMCID: PMC10353122
- DOI: 10.1186/s12967-023-04339-5
Unraveling the epigenetic landscape of pulmonary arterial hypertension: implications for personalized medicine development
Abstract
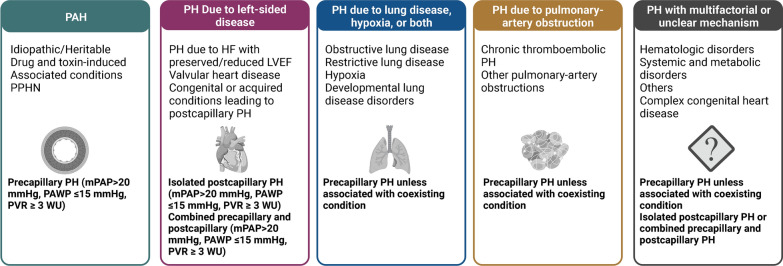
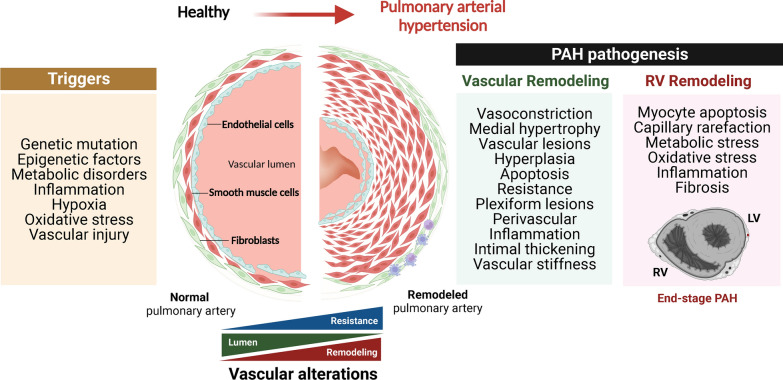
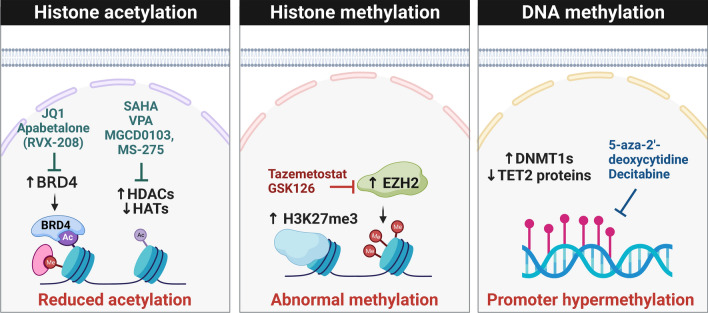
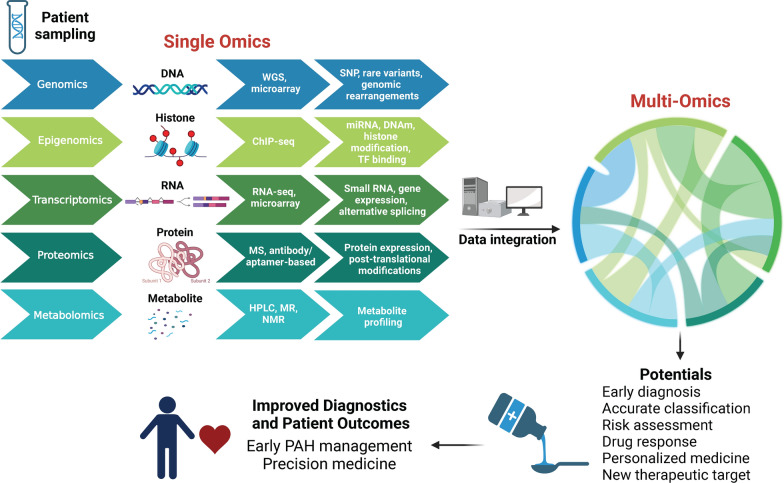
Pulmonary arterial hypertension (PAH) is a multifactorial disease associated with the remodeling of pulmonary blood vessels. If left unaddressed, PAH can lead to right heart failure and even death. Multiple biological processes, such as smooth muscle proliferation, endothelial dysfunction, inflammation, and resistance to apoptosis, are associated with PAH. Increasing evidence suggests that epigenetic factors play an important role in PAH by regulating the chromatin structure and altering the expression of critical genes. For example, aberrant DNA methylation and histone modifications such as histone acetylation and methylation have been observed in patients with PAH and are linked to vascular remodeling and pulmonary vascular dysfunction. In this review article, we provide a comprehensive overview of the role of key epigenetic targets in PAH pathogenesis, including DNA methyltransferase (DNMT), ten-eleven translocation enzymes (TET), switch-independent 3A (SIN3A), enhancer of zeste homolog 2 (EZH2), histone deacetylase (HDAC), and bromodomain-containing protein 4 (BRD4). Finally, we discuss the potential of multi-omics integration to better understand the molecular signature and profile of PAH patients and how this approach can help identify personalized treatment approaches.
Keywords: Epidrugs; Epigenetic; PAH; Pulmonary arterial hypertension; Treatment.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ling Y, Johnson MK, Kiely DG, Condliffe R, Elliot CA, Gibbs JSR, Howard LS, Pepke-Zaba J, Sheares KKK, Corris PA, et al. Changing demographics, epidemiology, and survival of Incident Pulmonary arterial hypertension. Am J Respir Crit Care Med. 2012;186(8):790–6. doi: 10.1164/rccm.201203-0383OC. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
