

Health Care Costs Associated with the Development and Combination of Cardio-Renal-Metabolic Diseases
- PMID: 37461134
- PMCID: PMC10615376
- DOI: 10.34067/KID.0000000000000212
Health Care Costs Associated with the Development and Combination of Cardio-Renal-Metabolic Diseases
Abstract
Key Points:
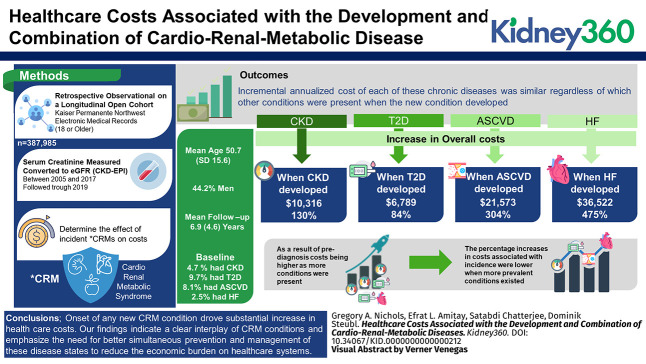
Onset of any new cardio-renal-metabolic condition drove substantial increase in health care costs.
Overall costs increased by $10,316 (130%) when CKD developed, $6789 (84%) for type 2 diabetes, $21,573 (304%) for atherosclerotic cardiovascular disease, and $36,522 (475%) for heart failure.
However, as a result of prediagnosis costs being higher as more conditions were present, the percentage increases in costs associated with incidence were lower when more prevalent conditions existed.
Background: The cardio-renal-metabolic (CRM) syndrome is a constellation of conditions which includes atherosclerotic cardiovascular disease, heart failure (HF), CKD, and type 2 diabetes. The economic consequences of developing each of these comorbidities in the context of the others have not been studied.
Methods: We used the electronic medical records of Kaiser Permanente Northwest to identify 387,985 members aged 18 years or older who had a serum creatinine measured between 2005 and 2017. Patients were followed through 2019. We used a statistical approach that assesses time dependency for continuous measures; the total observation period for each patient was divided into quarters (91-day increments), and each patient contributed a record for every quarter in which they were members of the health plan. CRM status was determined for each quarter.
Results: The incremental annualized cost of each of these chronic diseases was similar regardless of which other conditions were present when the new condition developed. Overall costs increased by $10,316 (130%) when CKD developed, $6789 (84%) for type 2 diabetes, $21,573 (304%) for atherosclerotic cardiovascular disease, and $36,522 (475%) for HF. However, as a result of prediagnosis costs being higher as more conditions were present, the percentage increases in costs associated with incidence were lower when more prevalent conditions existed.
Conclusions: Onset of any new CRM condition drove substantial increase in health care costs. Our findings indicate a clear interplay of CRM conditions and emphasize the need for better simultaneous prevention and management of these disease states to reduce the economic burden on health care systems.
Conflict of interest statement
E.L. Amitay reports the following: Employer: Boehringer-Ingelheim International GmbH. S. Chatterjee reports the following: Employer: S Chatterjee is an employee of Boehringer-Ingelheim Pharmaceuticals, Inc.; Research Funding: This research is sponsored by my current employer, Boehringer-Ingelheim; and Other Interests or Relationships: S. Chatterjee (self)—Adjunct Faculty appointment at the University of Houston College of Pharmacy, Department of Pharmaceutical Outcomes and Policy. This is an unpaid position, and involves serving as committee member in students' thesis and/or dissertation committees. G.A. Nichols reports the following: Research Funding: Boehringer Ingelheim. D. Steubl reports the following: Employer: Boehringer Ingelheim International GmbH.
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
