

The effect of adjuvant cryotherapy added to well-performed high-speed burr curettage on the long-term surgical outcomes of chondroblastoma cases
- PMID: 37462637
- PMCID: PMC10367154
- DOI: 10.52312/jdrs.2023.936
The effect of adjuvant cryotherapy added to well-performed high-speed burr curettage on the long-term surgical outcomes of chondroblastoma cases
Abstract
Objectives: This study aims to investigate the effect of adjuvant cryotherapy added to well-performed high-speed burr curettage on the long-term surgical outcomes of chondroblastoma cases.
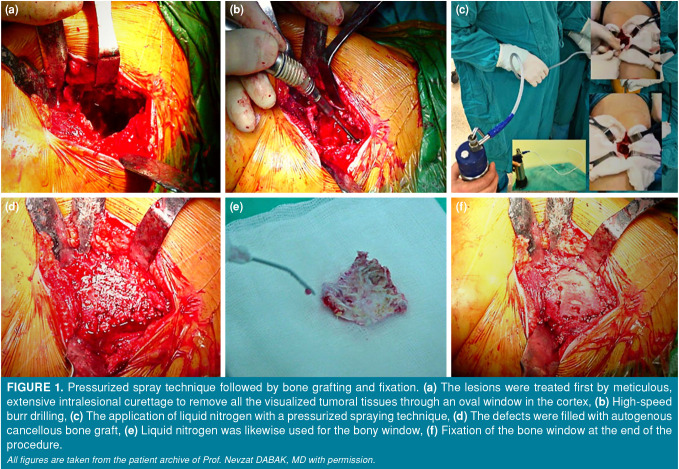
Patients and methods: Between January 2004 and December 2020, a total of 30 chondroblastoma cases (19 males, 11 females; median age: 18.6 years; range, 9 to 53 years) who were surgically treated were retrospectively analyzed. The pressurized-spray technique was performed using liquid nitrogen. Data including age, sex, radiological appearance, treatment modality, duration of follow-up, skin problems, and recurrence were recorded. All patients received adjuvant liquid nitrogen cryotherapy after extended intralesional curettage with high-speed burr. The bone cavity was filled with an autologous iliac crest bone graft, allograft, or polymethylmethacrylate (PMMA).
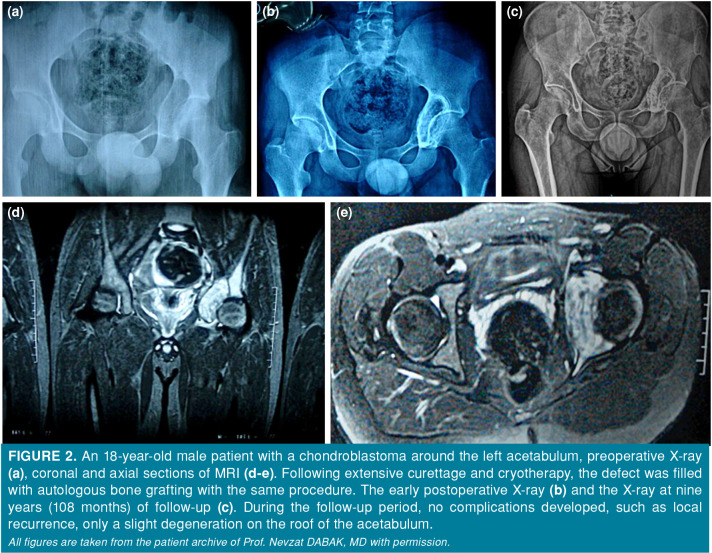
Results: The median follow-up was 54 (range, 19 to 120) months. The lesion was located around the knee in 16 (53.3%), in the shoulder in seven (23.3%), around the hip in five (16.6%), and in the ankle in two (6.6%) cases. The defect was filled with an autologous iliac crest bone graft in 28 (93.3%), an additional allograft in eight (26.7%), and PMMA in two (6.7%) cases. Local recurrence was observed in only two (6.7%) patients during follow-up. Two (6.7%) patients developed physeal growth arrest. Osteoarthritic changes were observed in two (6.7%) patients (one knee and one hip) due to the periarticular location of the tumor. Three (10%) patients had skin complications. None of the cases had a pathological fracture.
Conclusion: A well-performed extended intralesional curettage with high-speed burr is the first and essential step in treating chondroblastoma. Adding adjuvant liquid nitrogen cryotherapy with high-speed burr can improve treatment outcomes and significantly reduce the recurrence rate of this disease.
Conflict of interest statement
Figures
References
-
- Kolodny A. Bone sarcoma; primary malignant tumor of bone and giant cell tumor. Surg Gynecol Obstet. 1927;44:1–214.
-
- Mangham D. In: Mangham D. World Health Organisation classification of tumours. Pathology and genetics of tumours of soft tissue and bone. Christopher DM, Fletcher K, Unni K, Mertens F, editors. Lyon: IARC Press; 2004. pp. 427–427.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
