

A glycomic workflow for LC-MS/MS analysis of urine glycosaminoglycan biomarkers in mucopolysaccharidoses
- PMID: 37462780
- PMCID: PMC10638189
- DOI: 10.1007/s10719-023-10128-5
A glycomic workflow for LC-MS/MS analysis of urine glycosaminoglycan biomarkers in mucopolysaccharidoses
Abstract
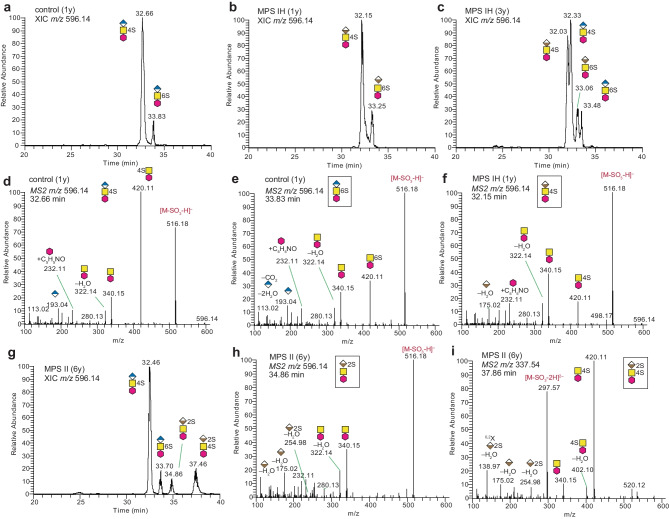
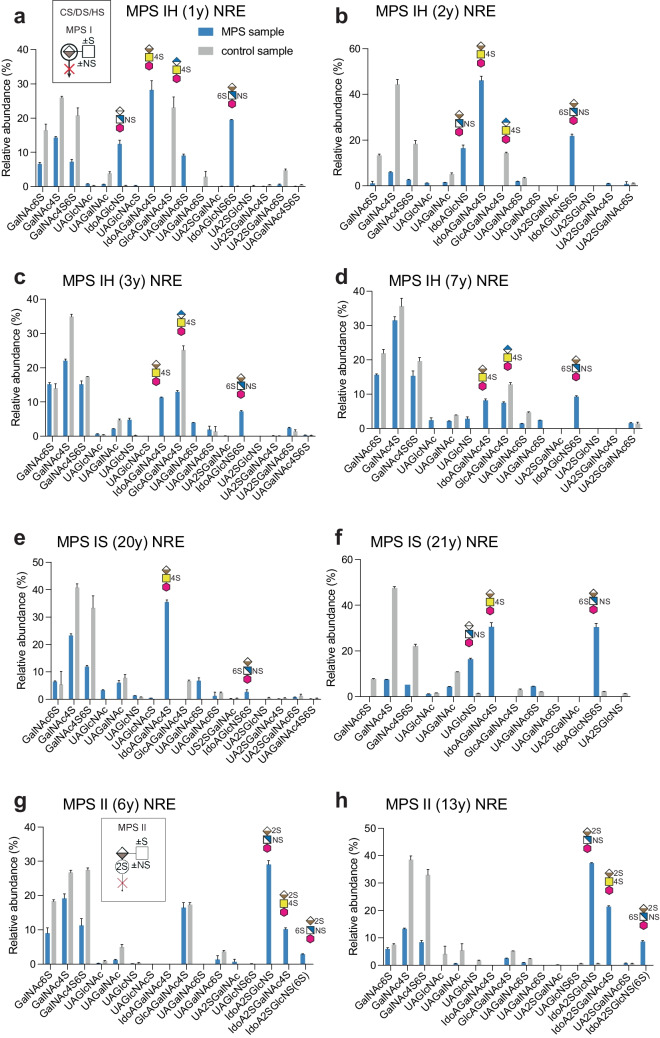
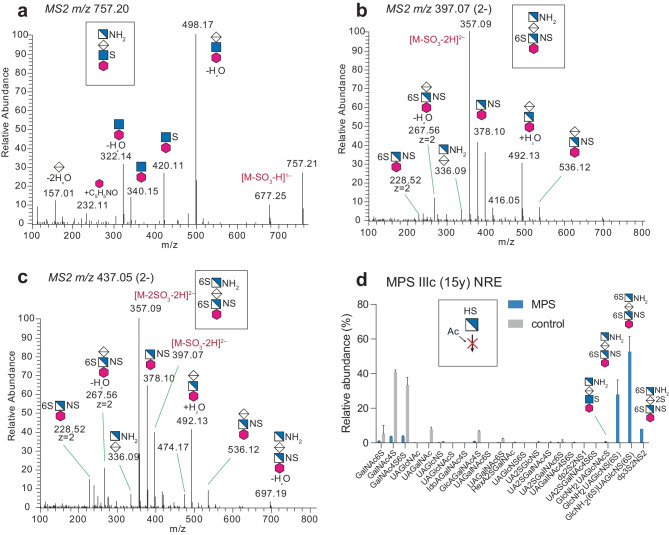
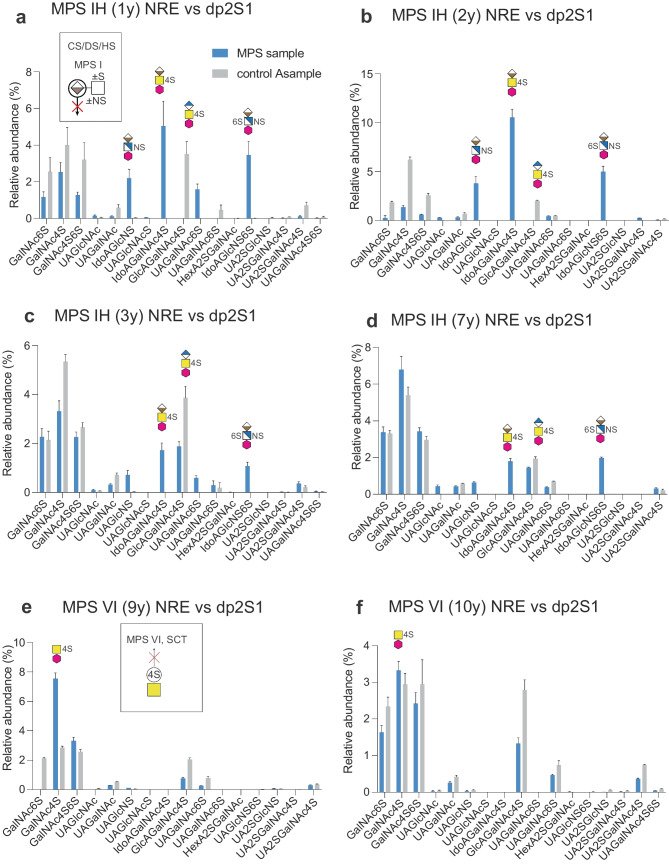
In recent years, several rational designed therapies have been developed for treatment of mucopolysaccharidoses (MPS), a group of inherited metabolic disorders in which glycosaminoglycans (GAGs) are accumulated in various tissues and organs. Thus, improved disease-specific biomarkers for diagnosis and monitoring treatment efficacy are of paramount importance. Specific non-reducing end GAG structures (GAG-NREs) have become promising biomarkers for MPS, as the compositions of the GAG-NREs depend on the nature of the lysosomal enzyme deficiency, thereby creating a specific pattern for each subgroup. However, there is yet no straightforward clinical laboratory platform which can assay all MPS-related GAG-NREs in one single analysis. Here, we developed and applied a GAG domain mapping approach for analyses of urine samples of ten MPS patients with various MPS diagnoses and corresponding aged-matched controls. We describe a nano-LC-MS/MS method of GAG-NRE profiling, utilizing 2-aminobenzamide reductive amination labeling to improve the sensitivity and the chromatographic resolution. Diagnostic urinary GAG-NREs were identified for MPS types IH/IS, II, IIIc, IVa and VI, corroborating GAG-NRE as biomarkers for these known enzyme deficiencies. Furthermore, a significant reduction of diagnostic urinary GAG-NREs in MPS IH (n = 2) and MPS VI (n = 1) patients under treatment was demonstrated. We argue that this straightforward glycomic workflow, designed for the clinical analysis of MPS-related GAG-NREs in one single analysis, will be of value for expanding the use of GAG-NREs as biomarkers for MPS diagnosis and treatment monitoring.
Keywords: Biomarkers; GAG-non-reducing ends; Glycomic; Glycosaminoglycans; Mucopolysaccharidosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare they have no financial interests. MB has given lectures in symposia and expert meetings sponsored by Sanofi Genzyme, Takeda Pharmaceutical Company and Biomarin Pharmaceutical, receiving no financial compensation.
Figures


References
-
- Verheyen S, Blatterer J, Speicher MR, Bhavani GS, Boons GJ, Ilse MB, Andrae D, Spross J, Vaz FM, Kircher SG, Posch-Pertl L, Baumgartner D, Lubke T, Shah H, Kaissi A, Girisha A, Plecko KM. Novel subtype of mucopolysaccharidosis caused by arylsulfatase K (ARSK) deficiency. J. Med. Genet. 2022;59(10):957–964. doi: 10.1136/jmedgenet-2021-108061. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
